Download
1 / 62
620 likes | 635 Views
Diagnosis: EBM Approach. Michael Brown MD Grand Rapids MERC/ Michigan State University. Scenario. 1 day colicky pain with nausea diffuse to RLQ mild tenderness, T 37. Step 1: Clinical Question.

E N D
Diagnosis: EBM Approach Michael Brown MD Grand Rapids MERC/ Michigan State University
Scenario • 1 day colicky pain with nausea • diffuse to RLQ • mild tenderness, T 37
Step 1: Clinical Question • In the patient presenting to the ED with suspected appendicitis, what is the accuracy of helical CT ?
Step 2: Search • MeSH Browser • appendicitis AND • computerized tomography AND • sensitivity and specificity • Clinical Query • diagnosis
Step 3: Critical Appraisal • Internal Validity • Results (focus today) • even if critical appraisal not your bag • External Validity
Evidenced-based Medicine • stresses methodology • de-emphasizes statistics • simplify: NNT, LR
Examples • Appendicitis • Pulmonary embolism • JAMA series • current slant
Threshold Approach to Clinical Decision Making • Treatment threshold • if above, start therapy • Test threshold • if below, no further testing Pauker NEJM 1980
Diagnostic Testing • Treatment threshold for PE? • If above: heparin • Test threshold for PE? • If below: discharge home • If between? • Further testing
LR post-test prob prior probability (predictive value) (prevalence)
Pretest Probability • experience in your setting • patient population • prevalence of condition in literature • Oxford web site • scoring systems
Estimate Pretest Probability for PE • history • risk factors • physical exam • initial screening tests
Estimate Pretest Probability for PE • Not exact science • usually a range 40-60% • low, intermediate, high • done daily in clinical practice • clinical prediction rules • physicians estimate very close Wicki 2001
Bayesian Analysis? • Thomas Bayes 1702-1761 • English clergyman • Doctrine of Chances
Bayesian Analysis • pretest probability • prevalence • LR for diagnostic test result • post-test probability • predictive value
Interpretation • convert pretest prob to odds • odds x LR = post-test odds • convert odds back to prob
Interpretation • convert pretest prob to odds • odds x LR = post-test odds • convert odds back to prob
Effect on pretest probability: • >10 or <0.1 large changes • 5-10 and 0.1-0.2 moderate • approach 1 no effect
Advantages of LR: • combines sensitivity and specificity • interpret test result on individual patient • multiple cut-offs • sequential testing
Shortcut: LR for + test = sensitivity 1 - specificity
Calculate: LR= prob (test result) with disease prob (test result) without disease
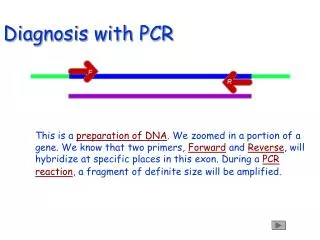
CT and Appendicitis Funaki et al
CT and Appendicitis • probability of + CT with appendicitis 29/30 = .97
CT and Appendicitis • Likelihood of + CT with appendicitis 29/30 = .97 • Likelihood of +CT without appendicitis 4/70 = .057 • LR for + CT = 17
Effect on pretest probability: • >10 or <0.1 large changes • 5-10 and 0.1-0.2 moderate • approach 1 no effect
Scenario • 1 day colicky pain with nausea • diffuse to RLQ • mild tenderness, T 37 • Pretest probability 30% • range 20 - 40%
Effect on pretest probability: • >10 or <0.1 large changes • 5-10 and 0.1-0.2 moderate • approach 1 no effect
Advantages of LR: • combines sensitivity and specificity • interpret test result on individual patient • multiple cut-offs • don’t have to lump! • sequential testing
Calculate: LR= prob equivocal CT with disease prob equivocal CT without disease
normal low prob intermediate prob high prob LR 0.1 LR 0.4 LR 1 LR 18 Multiple cut-offs: V/Q scan JAMA series
Sequential Testing • post-test probability 1st test • new pretest probability for 2nd test • assume independence
CT + CT - LR 8 LR .2 Helical CT : Diagnosis of PE Rathbun, 2000
> 500 <500 LR 2 LR .1 ELISA D-dimer: Diagnosis of PE Brown, Bermingham 2001