Download
1 / 49
510 likes | 896 Views
31:128 Psychopharmacology Professor A. K. Johnson Spring 2012 Unit 6: Outline CNS Neurodepressants and Sedative-Hypnotics. I. Introduction II. Amino Acid Neurotransmitters A. Glutamate: Excitatory amino acid (EAA) neurotransmitter 1. Glutamine synapse 2. Metabolism of glutamate

E N D
31:128 PsychopharmacologyProfessor A. K. JohnsonSpring 2012Unit 6: OutlineCNS Neurodepressants and Sedative-Hypnotics I. Introduction II. Amino Acid Neurotransmitters A. Glutamate: Excitatory amino acid (EAA) neurotransmitter 1. Glutamine synapse 2. Metabolism of glutamate 3. EAA neurotransmitters in the brain 4. EAA neuronal injury and death B. GABA: An inhibitory amino acid neurotransmitter 1. GABA synapse 2. Metabolism of GABA 3. GABA pathways in the brain 4. GABA receptor subtypes III. Neurodepressants and Sedative-Hypnotics A. Therapeutic uses of sedative-hypnotics and anxiolytics B. Classification of sedative-hypnotics/anxiolytics C. Barbiturates D. Benzodiazepines E. Non-barbiturate/non-benzodiazepine sedative-hypnotics/anxiolytics IV. Alcohol A. Sources B. Pharmacokinetics 2830/6.0
CNS Neurodepressants and Sedative-Hypnotics(Continued) C. Behavioral and physiological effects/dose-response D. Side effects of alcohol E. Alcohol and drug interactions F. Alcohol abuse G. Fetal alcohol syndrome V. Epilepsy A. The nature of epilepsy B. Electrophysiological correlates of epilepsy C. Pharmacological treatment of epilepsy D.Cellular mechanisms of antiepilepsy drugs 1. Na+ and Ca2+channel blockers 2. GABA agonists VI. Treatment of Sleep Disorders A. Common sleep disorders B. Benzodiazepines C. Non-benzodiazepine therapeutics 2830/6.0b
Key Terms and Concepts AMPA Anxiolytics Excitatory amino acid neurotransmitters GABAergic synapse Glutamate recognition site Glutamatergic synapse Glycine site Kainate Metabotropic Mg2+ site NMDA PCP site Sedative-hypnotics Important Drugs and Chemicals -aminobutyric acid (GABA) Acetaldehyde Alcohol dehydrogenase Aldehyde dehydrogenase Baclofen Barbiturate site BDZ agonist (Diazepam) BDZ antagonist (Flumazenil) BDZ inverse agonist Benzodiazepine (BDZ) Bicuculline Buspirone Chloral hydrate Chlordiazepoxide Diazepam Disulfiram Ethanol GABA aminotransferase (GABA-T) Glutamate Glutamate acid decarboxylase (GAD) Isoguvacine Muscimol NAD NADH Oxazepam Pentobarbital Pentylenetetrazol Phenobarbital Picrotoxin Secobarbital Steroid site Thiopental 2830/6 KTC
Unit 5: CNS Neurodepressants and Sedative-Hypnotics Study Questions • What does excitatory vs. inhibitory amino acids mean? • Why do some amino acids cause excitation and others inhibition? • Describe the locations of the synthesis storage and degradation of glutamate. • How does glutamate cause neuronal injury? • What other agents act on GABAA receptors and why is this important? • List the various classes of CNS depressants and give examples of each class. What are common terms for CNS depressants? • What are the consequences of the drug blockade of glutamate receptors? Of GABA receptors? • Describe the consequences of a person taking progressively larger doses of a non-selective CNS depressant. 9. What is meant by cross-tolerance of CNS depressants? Why does it occur? 10. What mechanisms are responsible for the differing durations of action of various barbiturates? 11. What are the oldest CNS depressants? The newest? 12. Why might antiepileptic drugs be considered for use in non-epileptic, psychological disorders? 2830/6 Qa
Unit 5: CNS Neurodepressants and Sedative-Hypnotics Study Questions (continued) 13. What are the advantages of benzodiazepines over barbiturates? 14. Describe the mechanism of action of benzodiazepines. 15. Describe the structure and function of the benzodiazepine receptor. 16. List some of the clinical uses of benzodiazepines. 17. What is flumazenil and for what purpose can it be used? 18. Pharmacologically, what is ethyl alcohol? 19. Describe the metabolism of alcohol. What enzymes are involved? What drug blocks one of these enzymes? 20. How do women and men differ in their metabolism of alcohol? 21. Describe how alcohol exerts its effects on the CNS 22. If one has developed a physical dependence on alcohol, why might he or she be treated with a benzodiazepine as a substitute for the alcohol? 23. Describe some of the fetal effects of alcohol. Is there a "safe" level of drinking during pregnancy? 2830/6 Qb
The Glutamatergic Synapse 2830/6.1
• It is localized presynaptically in specific neurons where it is stored and released from synaptic vesicles. • It is released by a calcium-dependent mechanism by physiologically relevant stimuli in amounts sufficient to elicit postsynaptic responses. • A mechanism (reuptake) exits that will rapidly terminate its transmitter action. • It demonstrates pharmacological identity with the naturally occurring transmitter. • Receptors The Criteria Glutamate Has Met To Be Considered as a Neurotransmitter 2830/6.2
Proposed Pathways Using ExcitatoryAmino Acid Neurotransmitters 2830/6.3
Properties Receptor Subtypes Superfamily Genes Cation Selectivity 2nd Messengers AMPA Ligand-gated channel GluR1-GluR4 Na+, K+ Kainate Ligand-gated channel GluR5-GluR7, KA1 KA2 Na+, K+ NMDA Ligand-gated channel NR1, NR2A, NR2D Na+, K+, Ca2+ Metabotropic G protein-coupled mGluR1-mGluR7 IP3, DAG, cAMP receptor Structural and Functional Properties of Excitatory Amino Acid Receptors 2930/6.4
Schematic Representationof the NMDA Receptor Complex 2830/6.5
Biochemical Processes Hypothesized to Underlie Ischemic Neuronal Injury and Death 2830/6.6
The GABA Synapse 2830/6.7
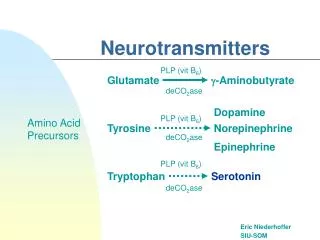
COOH COOH CH2 CH2 Glutamic Acid + CO2 CH2 Decarboxylase CH2 H2N CH H2N CH2 COOH Glutamate GABA GABA Synthesis 2830/6.8
The Interplay Between Neuronsand Glia in GABA Metabolism 2830/6.9
•Immunohistochemical localization of glutamic acid decarboxylase (GAD). •Immunohistochemical localization of GABA itself. •Histochemical localization of the GABA-destroying enzyme GABA aminotransferase (GABA-T). •Uptake of labeled GABA followed by autoradiography. Techniques Used to Localize GABA Pathways 2830/6.10
Substance Brain Region (Species) Peptide Somatostatin Thalamus (cat) Cortex, hippocampus (rat, cat, monkey) CCK Cortex, hippocampal formation (cat, monkey, rat) NPY Cortex (cat, monkey) Enkephalin Retina (chicken) Ventral pallidum, hypothalamus (rat) Opioid peptide Basal ganglia (rat) Galanin Hypothalamus (rat) Substance P Hypothalamus (rat) VIP Hippocampal formation (rat) Classical Transmitter 5-HT Nucleus raphe dorsalis (rat) Medullary raphe nuclei and adjacent areas (rat) Retina (rabbit) DA Arcuate nucleus (rat) Olfactory bulb (rat) Histamine Hypothalamus (rat) ACh Medial septum/diagonal band (rat) Glycine Cerebellum (rat) Colocalization of GABA with ClassicalTransmitters and Peptides in the Mammalian CNS CCK, cholecystokinin; NPY, neuropeptide Y; VIP, vasoactive intestinal polypeptide; 5-HT, DA, dopamine; ACh, acetylcholine. 2830/6.11
Schematic Model of the GABAA Receptor Complex BDZ, benzodiazepine 2830/6.12
•Insomnia •Anxiety •Epilepsy •Muscle spasticity •Induction of amnesia •As preanesthetic mediation •Adjunct in alcohol withdrawal Therapeutic Uses ofSedative-Hypnotics and Anxiolytics 2830/6.13
• Barbiturates - Thiopental - Secobarbital - Pentobarbital - Phenobarbital •Benzodiazepines - Chlordiazepoxide (Librium) - Diazepam (Valium) - Oxazepam - Others • Non-Barbiturates/Non-Benzodiazepines - Chloral hydrate - Carbamates (e.g., meprobamate) - Buspirone - Miscellaneous [e.g., ethchlorvynol; quinazolinone, (methaqualone); piperidinediones (methyprylon, glutethimide); -blockers (propranolol); 2-adrenergic receptor agonist (clonidine)] Classification ofSedative-Hypnotics and Anxiolytics 2830/6.14
A. Characteristics • all general, non-selective CNS depressants •relatively low therapeutic indices • drug interactions – induce liver enzymes • all derived from barbituric acid B. Absorption and Distribution • administered as water-soluble free acid •oral – when used to treat anxiety or sleep disorders • intravenously – when used as adjuncts to general anesthesia • thiobarbiturates are very lipid soluble and have a very rapid onset of action because of high rate of entry into CNS; but they also rapidly redistribute from CNS to highly perfused tissues and then to fat thus rapidly terminating their CNS effects. C. CNS Actions • decrease the amount of neurotransmitter released in excitatory neurons •barbiturates interact with GABA to enhance postsynaptic inhibition • increases the duration of GABA-Cl channel opening • depresses the reticular activating system and excitability of cortical cells •sedation – drowsy, aroused by external stimuli • hypnosis – sleep, aroused by external stimuli • coma – not aroused by external stimuli • death – not aroused by external stimuli •anticonvulsant action: best anti-epileptics are phenobarbital, mephobarbital and metharbital; they have rather selective actions as patient can be seizure-free and functional • analgesia – very weak or none D. Respiratory, Cardiovascular and Autonomic Effects • depress respiratory drive and rhythm •cross placental membrane and may depress fetal respiration • at sedative-hypnotic doses, there is only a slight fall in blood pressure and heart rate • blockade of sympathetic ganglionic transmission Barbiturates 2830/6.15
E. Cautions, Side Effects and Contraindications •spatial judgment impaired •drug interactions – augmentation of CNS depressive effects of ethyl alcohol; phenothiazine (antipsychotics); antihistamines; and antihypertensives •contraindicated in certain pathological states (e.g., pulmonary insufficiency and emphysema) •contraindicated in patients with previous allergic reactions •drug interactions - enzymes F. Tolerance •tolerance develops to the sedative-hypnotic effects of barbiturates •metabolic tolerance – enzyme induction •pharmacodynamic tolerance – adaptation of nervous tissue to drug presence G. Physical Dependence •large problem!! •withdrawal symptoms may be severe (e.g., seizures) H. Barbiturate Poisoning •moderate intoxication similar to alcoholic inebriation •symptoms of severe intoxication: coma – can last up to five days with phenobarbital; constricted pupils dilation due to hypoxia; breathing slow or rapid and shallow; shock syndrome may develop (fall in blood pressure) •death may be due to respiratory depression or complications of prolonged coma (pulmonary edema) •treatment – charcoal lavage; intensive support therapy (respiratory); no stimulants; hemodialysis Barbiturates (con't) 2830/6.16
Barbiturates:Duration of Action 2830/6.17
Tolerance and Therapeutic Index 2830/6.18
Effect of Chronic BarbiturateAdministration on Sleep Architecture 2830/6.19
Blood Levels of Secobarbital in Mothers and Newborn Infants 2830/6.19a
A. Characteristics • today, the most commonly used sedative - hypnotics B. Mechanism of Action • preferentially act on the limbic system (septum, amygdala and hippocampus) where they potentiate GABAergic inhibitory neurotransmission •increases the frequency of GABA-Cl channel opening C. Absorption and Distribution • benzodiazepines are weakly basic (therefore absorbed better in duodenum) •several are metabolized to active forms • the more lipophilic benzodiazepines have shorter onset and duration of action D. Biotransformation and Excretion Chlordiazepoxide Diazepam Clorazepate Demoxepam* Desmethyldiazepam* Oxazepam Alprazolam Flurazepam * Conjugation * Triazolam Lorazepam Urinary Secretion * = Active metabolites Formation of active metabolites may complicate the pharmacokinetic analysis of parent drug and produce cumulative effects. Benzodiazepines 2830/6.20
E. Advantages of Benzodiazepines Over Barbiturates •safer, higher therapeutic index •less depression of respiration •less induction of hepatic drug-metabolizing enzymes •slower development of tolerance •low risk of physical dependence, withdrawal symptoms not severe •less depression of REM sleep F. Major Therapeutic Uses 1. Chlordiazepoxide • anticonvulsant, muscle relaxing properties, sedative and hypnotic effects. Used primarily in anxiety and muscular-skeletal disorders, and alcohol withdrawal syndromes; premedical treatment to anesthesia •is used for treatment of prolonged anxiety, because of its long duration of action • is similar to meprobamate and barbiturates in general; cumulative effect and the withdrawal symptoms 2. Diazepam • an anticonvulsant and treatment of status epilepticus •used as an amnesic agent in dental surgery and for possible amnesic effects in procedures such as endoscopy and bronchoscopy • useful in acute alcohol withdrawal 3. Oxazepam • is an metabolite of diazepam with short duration of action G. Major Complications/Concerns •tolerance, physical dependence and cross tolerance occur with benzodiazepines and ALL other sedative-hypnotics including ethanol •tolerance is common and overdoses are frequent. However, serious consequences are rare. Treatment includes support of respiration and cardiovascular functions Benzodiazepines (con't) 2830/6.21
A. Chloral Hydrate • chemically reduced to the active metabolite in liver •the same sedative-hypnotic properties as barbiturates • currently used as pre-medication for children and elderly B. Carbamates - Meprobamate • possess sedative-hypnotic, anticonvulsant and muscle relaxing properties; used primarily in anxiety and muscular-skeletal disorders (e.g., muscle spasm); of no value in treating psychoses; suppresses REM sleep •ability to produce habituation and physical dependence similar to that for barbiturates; toxicity includes sleepiness, ataxia, hypotension; and massive overdose results in coma, shock, pulmonary edema and respiratory depression. The dose necessary to produce profound CNS depression is usually considered to be very much greater than that of a barbiturate • the drug should be withdrawn gradually and slowly • the locus and mechanism of action are unknown C. Buspirone ("Second Generation" Anxiolytic) • it is an effective anti-anxiety drug and is a 5-HT1A receptor agonist •has no effect on GABA or benzodiazepine binding • has little interaction with CNS depressants, but caution must be exercised with alcohol • possesses no anticonvulsant properties •has low risk of dependence • has no effect on panic disorder • elicits no cross tolerance with other anti-anxiety drugs Non-Barbiturates/Non-Benzodiazepine 2830/6.22
The Advantages of Drug "B" Over Drug "A" as Deduced From Dose-Response Curves 2830/6.23
Definitions and Recipes for Various Alcoholic Beverages Grain Neutral Spirits Flavorless alcohol of 190 proof or above. Used only in research and medicine or diluted in vodka or blended whiskeys to raise the alcohol content. Lager Beer From German lagern, to store. The species of yeast used sinks to the bottom of the mash. The beer is stored to age. Draft Beer Filtered at the end to remove the remaining active yeast, so the containers won't explode during shipping. Usually pasteurized. Ale Like beer, but it ferments at higher temperatures, using a yeast that floats in the mash. Has more malt, hops, and flavor than beer. Malt Liquor A beer aged like lager, it is carbonated and higher in calories and in alcohol (by 1%-3%). Sparkling Wine A white wine corked before the yeast dies, so that it becomes naturally carbonated by trapped C02. Varietal Wine Over half of the wine comes from a single species of grape. Generic Wine Blends of wines named after regions of Europe: Bordeaux, Burgundy, Rhine wine. Champagne White generic wines carbonated like sparkling wine. Brandy Distilled from wine or from a particular fruit wine, like cherry or peach brandy. Dessert Wine Fortified with brandy to raise the alcohol content to near 40 proof. Port and Madeira are most common. Liqueur A wine distilled and combined with herbs or other flavorings. Sugar content is high. Scotch Distilled from fermented barley malt, cooked over a peat fire, stored 3 years in uncharred barrels originally filled with sherry. Vodka From Russian, "a little water" (voda is water). Pure, almost 190 proof, alcohol diluted with water, and unaged. There is no difference between marketed vodkas except the proofs, the prices, or added flavorings. Rum Distilled from fermented sugar cane molasses. Gin Distilled from corn and water, filtered through juniper berries to soften the flavor and provide its distinctive taste. Whisky Distilled from rye or corn. Straight rye whisky has over 50% rye grain in the mash. Bourbon uses over 50% corn, and corn whisky over 80%. Rye and bourbon are diluted to between 120 and 125 proof and aged in new, charred oak barrels for two or more years. Bourbon gets its name from Elijah Craig, a minister in Bourbon Country, Kentucky, who developed this recipe. Congeners that accumulate during the first 5 years of aging make the taste. 2830/6.24
Time Course of Brainand Venous Ethanol Concentrations 2830/6.25
Relationship Between Blood Alcohol Concentration and Signs of Intoxication 2830/6.26
Metabolism of Ethanol and the Use of the Aldehyde Dehydrogenase Inhibitor, Disulfiram 2830/6.27
Dose-Blood Level-Response for Alcohol Ethanol Dose Blood Ethanol Function Impaired Physical State(oz/hour) (mg/100 ml) 1-4 up to 100 judgment happy fine motor coordination talkative reaction time boastful 4-12 100-300 motor coordination staggering reflexes slurred speech nausea, vomiting 12-16 300-400 voluntary responses to hypothermia stimulation hyperthermia anesthesia 16-24 400-600 sensation comatose movement self-protective reflexes 24-30 600-900 breathing dead heart function 2830/6.28
Effects and Side Effects of Ethanol* Side Effects Possible Mechanism/Cause Reduced neuronal conduction Increased membrane fluidity Sedation Benzodiazepine-independent enhancement ofIncreased seizure threshold GABA functionAnterograde amnesia Euphoria Delta opioid-like effectsMemory impairment Acetylaldehyde conjugation with CAs toAnalgesia produce conjugates with opiate-like effectsSedation and neuronal damage Blood pressure alterations Acute release of CAs/CNS depressionDependence liability Increased DA in n. accumbensVasodilation Smooth-muscle relaxation/peripheral neuropathy Sedation Anticholinergic effectsMemory impairmentDelirium Anxiolysis Altered 5-HT function; GABA actionsSedationMood alterations Peripheral neuropathy Thiamine deficiency (poor diet) Cirrhosis NAD depletion; astringent actions/reducedGI problems juices/reduced water-soluble vitamin absorption Cardiac disease Alterations in HDL, increased heart work, alcohol-mediated cardiomyopathy Reduced ADH release Depression of hypothalamus Reduced body temperature Depression of hypothalamus and peripheral vasodilation Fetal alcohol syndrome Dietary problems, reduced vitamin absorption, direct effects of alcohol on fetal brain *CA = catecholamines; NAD = nicotine-adenine dinucleotide; ADH = antidiuretic hormone; HDL = high-density lipoprotein 2830/6.29
This chart lists classes of drugs that have been reported to interact with alcohol. Some of the dangers that may result from combining alcohol with the other listed drugs are described. It must be emphasized that this chart, or any other like it, represents only the smallest part of the whole alcohol/drug interaction picture. Antihistamines (most cold remedies, Actifed, Coricidin, etc.)Taking alcohol with this class of drugs increases their calming effect, and a person can feel quite drowsy, making driving and other activities that require alertness more hazardous. Antihypertensive Agents (Serpasil, Aldomet, Esidrix, etc.)Alcohol may increase the blood pressure lowering capability of some of these drugs, causing dizziness when a person get up. Antiinfective Agents/Antibiotics (Flagyl, Chloromycetin, Seromycin, etc.)In combination with alcohol, some may cause nausea, vomiting, and headache, and possibly convulsions, especially those taken for urinary tract infections. Some are rendered less effective by chronic alcohol use. Central Nervous System Stimulants (most diet pills, Dexedrine, Caffeine, Ritalin, etc.)Because stimulant effect of this class of drugs may reverse the depressant effect of the alcohol on the central nervous system, these drugs can give a false sense of security. They do not help intoxicated persons gain control of their movements. Diuretics (Diuril, Lasix, Hydromox,, etc.)Combining alcohol with diuretics may cause reduction in blood pressure possibly resulting in dizziness when a person stands up. Sleep MedicinesIt is likely that nonprescription sleeping medicines, to the degree that they are effective, will lead to the same kind of central nervous system depression when combined with alcohol as the minor tranquilizer (see below). Tranquilizers (Miltown, Valium, Librium,, etc.)Tranquilizers in combination with alcohol will cause reduced functions of the central nervous system, especially during the first few weeks of drug use. This results in decreased alertness and judgment, and can lead to household and automotive accidents. VitaminsContinuous drinking can keep vitamins from entering the bloodstream. However, this situation changes when a person stops drinking. Why Drinks and Drugs Don't Mix Analgesics, Narcotic (Demerol, Codeine, Percodan, etc.)When used alone, either alcohol or narcotic drugs cause a reduction in the function of the central nervous system. When they are used together, this effect is even greater and may lead to loss of effective breathing function (respiratory arrest). Death may occur. Analgesics, Non-Narcotic (Aspirin, Tylenol, Pabalate, etc.)Even when used alone, some nonprescription pain relievers can cause bleeding in the stomach and intestines. Alcohol also irritates the stomach and can aggravate the bleeding, especially in ulcer patients. Alcohol may also increase susceptibility to liver damage from acetaminophen. Antialcohol Preparations (Antabuse)Use of alcohol with medications prescribed to help alcoholic patients keep from drinking results in nausea, vomiting, headache, high blood pressure, and possible erratic heartbeat; and can result in death. Anticoagulants (Panwarfin, Dicumarol, etc.)Alcohol can increase the ability of these drugs to stop blood clotting, which in turn can lead to life-threatening or fatal hemorrhages Anticonvulsants (Dilantin)Drinking may lessen the ability to these drugs to stop convulsions and may exaggerate blood disorder side effects of the anticonvulsant. Antidepressants (Tofranil, Pertofrane, Triavil, etc.)Alcohol may cause an additional reduction in central nervous system functioning and lessen a person's ability to operate normally. Certain antidepressants in combination with red wines like Chianti may cause a high blood pressure crisis. Psychotropics (Sparine, Mellaril, Thorazine, etc.)Alcohol with the "major tranquilizers" causes additional depression to central nervous system function, which can result in severe impairment of voluntary movements such as walking or using the hands. The combination can also cause a loss of effective breathing function and can be fatal. Sedative Hypnotics (Doriden, Dalmane, Nembutal, Quaalude, etc.)Alcohol in combination further reduces the function of the central nervous system, sometimes to the point of coma or the loss of effective breathing (respiratory arrest). This combination can be fetal. Antidiabetic Agents/Hypoglycemics (Insulin, Diabinese, Orinase, etc.)Because of the possible severe reactions to combining alcohol and insulin or the oral antidiabetic agents, and because alcohol interacts unpredictably with them, patients taking any of these medications should avoid alcohol. 2830/5.30
Alcohol (ETOH) Use and Abuse In U.S. nearly 75% of all adults drink ETOH. 15% of ETOH users in the U.S. are considered to have a drinking problem or are subject to alcoholism. 10 million Americans are classified as alcoholics. Alcoholism is most severe of all substance abuse in USA. More people become dependent on ETOH, become psychotic through excessive use of it and are killed or disabled by it than by all other abused drugs (except nicotine via tobacco) put together. 11 million accidents each year are ETOH-related. Alcoholism costs the U.S. economy $136 billion. 2830/6.31
American Medical AssociationDefinition of Alcoholism Alcoholism is an illness characterized by preoccupation with alcohol and loss of control over its consumption such as to lead usually to intoxication if drinking is begun; the condition is chronic, progressive, and has a tendency toward relapse. It is typically associated with physical disability and impaired emotional, occupational, and/or social adjustments as a direct consequence of persistent and excessive use of alcohol. 2830/6.32
Children with Fetal Alcohol Syndrome (FAS) Compared with a Mouse Model of FAS FAS Signs and Symptoms 1. Mental retardation and developmental delays 2. Low birthweight 3. Neurological disorders (tremor, irritability auditory hypersensitivity, etc.) 4. Craniofacial malformations 5. Assorted physical abnormalities 2830/6.33
CNS Neurodepressants and Sedative-Hypnotics(Continued) V. Epilepsy A. The nature of epilepsy B. Electrophysiological correlates of epilepsy C. Pharmacological treatment of epilepsy D. Cellular mechanisms of antiepilepsy drugs 1. Na+ and Ca2+channel blockers 2. GABA agonists VI. Treatment of Sleep Disorders A. Common sleep disorders B. Benzodiazepines C. Non-benzodiazepine therapeutics 2830/6.34
Nature of Epilepsy Epilepsy affects about 0.5% of the population. The characteristic event is the seizure, which is often associated with convulsions, but may occur in many other forms. The seizure is caused by an abnormal high frequency discharge of a group of neurons, starting locally and spreading to a varying extent to affect other parts of the brain. Seizures may be partial or generalized depending on the location and spread of the abnormal neuronal discharge. The attack may involve mainly motor, sensory or behavioral phenomena. Unconsciousness occurs when the reticular formation is involved. Partial seizures are often associated with damage to the brain, whereas generalized seizures occur without obvious cause. Two common forms of generalized epilepsy are the tonic-clonic fit (grand mal) and the absence seizure (petit mal). The neurochemical basis of the abnormal discharge is not well understood. It may be associated with enhanced excitatory amino acid transmission, impaired inhibitory transmission, or abnormal electrical properties of the affected cells. Prolonged epileptic discharge (status epilepticus) can cause neuronal death (excitotoxicity). Current drug therapy is effective in 70-80% of epileptic patients. 2830/6.35
Relations Among Cortical EEG, Extracellular, and Intracellular Recordings in a Seizure 2830/6.37
Pharmacological Treatment of Epilepsy Agents Acting to: Enhance Na+ Channel Inactivation Phenytoin Carbamazepine Valproate Enhance GABAergic Transmission Phenobarbital Clonazepam Vigabatrin Tiagabine Gabapentin Inhibit Ca2+ Channels Ethosuximide 2830/6.38
Antiseizure Drug-Enhanced Na+ ChannelInactivation (Top) and Drug-Induced Reductionof Current Through T-Type Ca2+ Channels 2830/6.39
Enhanced GABA Synaptic Transmission 2830/6.40
Comparison of Representative Benzodiazepines for Insomnia Therapy 2830/6.42
Non-Benzodiazepine Therapy for Insomnia 2830/6.43