Download
1 / 52
520 likes | 802 Views
Leprosy genetics susceptibility and resistance. Prepared by: - Ilham Abd Allah EL- bushra - Safaa Othman Andarawi. CONTENT. Introduction to leprosy Genome wide scan Candidate genes:- HLA genes Non-HLA genes.

E N D
Leprosy genetics susceptibility and resistance Prepared by: - IlhamAbd Allah EL-bushra - Safaa Othman Andarawi
CONTENT • Introduction to leprosy • Genome wide scan • Candidate genes:- • HLA genes • Non-HLA genes
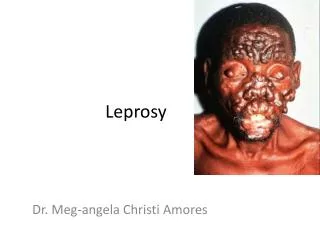
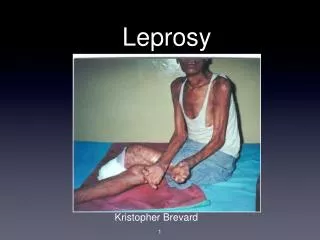
Leprosy is a chronic infectious disease caused by the organism Mycobacterium leprae. • Leprosy is primarily a disease of the peripheral nerves and mucosa of the upper respiratory tract, skin lesions are the primary external symptom. • it has long been recognized that leprosy clusters in families and it is often regarded as genetic disease
Evidence suggests that the incidence of leprosy infection is much higher than the incidence of clinical leprosy. • Only a small proportion (about 5%) of those infected are thought to develop clinical symptoms; This may be due in part to environmental factors but there is also a wealth of evidence for a genetic basis for host susceptibility to both disease per se and diseases sub-type. (M-A Shaw1,2,)
Who is at risk of leprosy? • Leprosy can affect people of all races all around the world. However, it is most common in warm, wet areas in the tropics and subtropics. • Worldwide prevalence is reported to be around 5.5 million, with 80% of these cases found in 5 countries: India, Indonesia, Myanmar, Brazil and Nigeria. • Leprosy presents most often during two different periods of life, between the ages of 10 and 14 and in those aged 35-44 years old. It is rarely seen in infants.( Vanessa Ngan2009)
Classification of leprosy: • classic classification system for leprosy clinical forms was • proposed in 1966 by Ridley and Jopling . Five groups of leprosy cases spanning the entire disease spectrum : • tuberculoid (TT), borderline tuberculoid (BT), midborderline(BB), borderline lepromatous (BL) and lepromatous(LL) leprosy. • More recently, a treatment-oriented system created by WHO classifies leprosy patients into three groups.: • Patients presenting a single skin lesion are classified as • single-lesion paucibacillary cases, paucibacillary leprosy (PB) includes all cases presenting five or fewer skin lesions
Classification of leprosy: (S. L. Walker.et al.2006)
Classification of leprosy: • patients presenting six or more skin lesions plus detectable M. leprae are classified as multibacillary (MB). • When comparing the two systems: • the single and multi-lesion PB patients are generally equivalent to the TT , BT. • while MB patients represent BB , BL , LL disease of the Ridley and Jopling system.
Genetics of susceptibility • Epidemiological and clinical observations suggested that the disease does not occur in most of the exposed individuals, Thus, the vast majority of people have some sort of innate resistance that can be, explained by their genetic background. There is a large evidence indicating genetic influence in leprosy outcome, suchas • (i) familial clustering; • (ii) distinct prevalence rates associated with distinct ethnic groups in an endemic area with similar exposure to the infectious agent; • (iii) high-throughput sequencing data from M. leprae genomes suggest that this pathogen has a very low genetic diversity,indicating a crucial role for the host genetics in disease outcome. • (Kerrie Tosh,et al .2002)
Genetics of susceptibility Genetics of susceptibility • The suggestion that leprosy is a hereditary disease dates back to the Middle Ages. • Modern scientific investigation of the hypothesis of a genetic component for human susceptibility to leprosy started at the turn of the nineteenth century with the first reports of leprosy occurrence among twins. Twin studies in India demonstrated higher concordance rates for leprosy in monozygotic twins (60%–85%) than in dizygotic twins (5%–20%) (M.R.Chakravartti,1937) . • Complex segregation analyses have found models consistent with a single major codominant or recessive gene and perhaps several modifying genes controlling susceptibility to leprosy in some populations
Leprosy in Sudan • Socio-cultural aspects of leprosy among the Masalit and Hawsa tribes in the Sudan. • The target populations were Masalit and Hawsa, the two main tribes in the area. Knowledge about the pathological cause of leprosy was lacking but the clinical manifestations were well recognized, particularly among the Masalit, in whom the disease is more common than the Hawsa. Among the Masalit there was a widely held belief that leprosy was caused by eating meat of the wild pig and a certain type of fish. The Hawsa, who are more devout Muslims, do not eat pig and associate leprosy with consumption of two types of fish. Between both tribes, the stigma of leprosy was not strong and the degree of rejection was more towards those with severe disease, particularly patients with ulcerated lesions and severe deformities. Patients were cared for by the family and lived in a separate hut within the families' housing compounds
Chromosome 10p13 Family study was done in south India ,all patients had been diagnosed as TT leprosy form.(M. Ruby Siddiqui1) .
Chromosome 6 p25 • In 197 Vietnamese families they found a significant association between leprosy and 17 markers located in the 5' regulatory region shared by PARK2 gene and the co-regulated gene PACRG.(mira mt 2004) • This was confirmed in a sample of 975 unrelated leprosy cases and controls from Brazil in whom the same alleles were strongly associated with leprosy. Variants in the regulatory region shared by PARK2 and PACRG therefore act as common risk factors for leprosy.
Chromosome20 • In 2002 asusceptibility locus in chromosome 20 was found in a study done in nourthindia in two ethnic group where the families show cluster of leprosy • It was a non parametric linkage study where : • 175 families (which included 185 independent affected sib pairs) were found in Sakthi Nagar and Kumbakonam in Tamil Nadu.58 other families (including 71 independent sib pairs) were found in Vizag in Andhra Pradesh. Both parents were available for study participation.
Chromosome 20 linkage map for families from Tamil Nadu, India. Single-point (solid line) and multipoint (broken line) maximumlogarithm of odds score (MLS) values are shown.
Mitsuda Reaction and Chromosomal Regions 2q35 and 17q21 • These region found to involved in the clinical out come of the infection with M.leprae, by controlling the formation of active granulomatus reaction • This was tested in a study done in Vietnam by doing the mitsuda reaction
Mitsuda reaction • The Mitsuda reaction is a granulomatous skin reaction, measured 21–30 days after the intradermal injection of 0.1 mL of lepromin (heat-killed M. leprae). The results of the Mitsuda test are classically interpreted as a binary outcome, either negative (<3 mm) or positive (>3 mm).
Mitsuda Reaction and Chromosomal Regions 2q35 and 17q21 • Many studies strongly suggested the presence of genetic components influencing Mitsuda-reaction values. • The first study was a candidate-gene study that showed evidence for linkage between Mitsuda reactivity and the SLC11A1 gene (also known as“NRAMP1”) in a population from Vietnam (Alcaı¨s A,ET AL 2000) • The latest one was a genome wide linkage scan in a sample of families from Vietnam.( Brigitte R.et al,2007)
MHC region susceptibility to leprosy • Association and Linkage analysis of leprosy phenotypes with HLA class II and TNF genes performed in brazilian population found the significant linkage between HLA class II region (HLA-DQB1 ,HLA-DQA1) and HLA-DRB1) • Linkage was also found to the TNF locus(LOD = 4.000, P = 0.00002).
MHC Region Study In India South Indian families, consisting of sib pairs with mainly(TT) form of disease. were genotyped at the DRB1 and DQB1 loci of HLA, the TNF-308 promoter polymorphism ,(LTA) gene, MICA and MICB gene (Muthuswamy Ravikumar 2006).
Continue ….. • in numerous case control studies DQ alleles especially DQw1 have been shown to be associated with tuberculoid leprosy in India, Korea, Thailand and Japan, and with lepromatous leprosy in India and Japan. (Wellcome Trus 2002) • (Rani et al.17 2007) confirmed by molecular typing, and reported association of DRB1*1501 with leprosy susceptibility, whereas DRB1*04 and DRB1*07 were associated with resistance to leprosy. In addition, HLA-DR3 has been found associated with leprosy susceptibility in Surinam and Mexico.
Continue ….. • A small study of leprosy cases and controls in Southern China suggested that an exon 5 variant of the MICA gene may be associated with resistance to multibacillary form of the disease.
TLR2 TLR2: • 86 Korean leprosy patients were screened for polymorphisms in a highly conserved part of the TLR2 intracellular domain. C to T substitution that results in an arginine to tryptophan change at the highly conserved amino acid 677 was found in 22% of the 45 lepromatous leprosy patients (J Fitness 2002) TLR2 polymorphisms are
Continue TLR-2 • Three polymorphisms in TLR2 (597C3T, 1350T3C, and a microsatellite marker) were analyzed in 431 Ethiopian patients withleprosy and 187 control subjects.result in , The microsatellite and the 597 T polymorphisms both influenced susceptibility to reversal reaction. (Marta Janer2008)
VitaminDreceptor (VDR) Vitamin D receptor (VDR): The evidence for association of the VDR gene in leprosy was firstly reported in a study in an Indian population (Bengalis), testing for a T-C substitution at codon 352.(OR 1.67; P value 0.03. This work detected susceptibility to lepromatous and tuberculoid leprosy in the presence of genotypes TT and CC respectively. a larger case-control study conducted in Malawians reported susceptibility to leprosy per se in the presence of the CC genotype. (M. O. 198 Moraes et al).
IL-10 interleukin-10 has many effects upon the functions of cells such as lymphocytes, monocytes, natural killer cells, and dendritic cells. Specifically, IL-10 is a cytokine that regulates immune-mediated inflammation. It appears to have two major functions: (1) to inhibit cytokine (i.e., TNF, IL-1, chemokine, and IL-12) production by macrophages and (2) to inhibit the accessory functions of macrophages in T cell activation. IL-10 accomplishes the latter function through the reduced expression of MHC class II molecules and certain co-stimulators (e.g., B7). IL-10 down regulates T-helper 1 cytokines and costimulatory molecules on macrophages, contributing to the persistence of the pathogens. (AC Pereira ,et al.2009)
Association analysis (AC Pereira ,et al.2009)
Genotypic , allelic and carrier frequency of promoter IL-10 (AC Pereira ,et al.2009)
IL-10 (AC Pereira ,et al.2009)
Summery of meta analysis of case-control studies of IL-10 -819 (AC Pereira ,et al.2009)
IL-10 measurement in PBMC culture supernatants (AC Pereira ,et al.2009)
IL-10 measurement in PBMC culture supernatants (AC Pereira ,et al.2009)