Download
1 / 77
790 likes | 1.1k Views
Neil Mclean March 12, 2009. Nutrition in the ICU CBP. Case.

E N D
Neil Mclean March 12, 2009 Nutrition in the ICU CBP
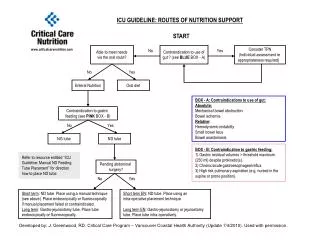
Case • You are working in the ICU and receive a patient from the OR. He is a 25 year old male who was involved in an MVC. His injuries include a severe closed head injury, a L hemopneumothorax with a chest tube in place, a splenic rupture (splenectomy performed) a grade 1 liver laceration, a L femur fracture (fixed). He is intubated and has an EVD in place. Upon admission, he is hemodynamically stable and you have done all the other right things. • You are now at the section in the pre-printed orders about options for feeding, You can choose between Parenteral Nutrition or Enteral Nutrition
Question #1 Does enteral nutrition compared to parenteral nutrition result in better results in critically ill adult patients? (MARIOS) Enteralvsparenteral nutrition in critically ill adult patients.
An ongoing saga… “…parenteral nutrition was an independent predictor of death (odds ratio of 2.09). The adverse sequelae associated with parenteral nutrition result from 1) not directly feeding the bowel; 2) the metabolic, immunologic, endocrine, and infective complications associated with parenteral nutrition; and 3) the fact that parenteral nutrition is infused into the patient’s systemic venous system, bypassing the liver.” Critical Care Medicine, 36(6) pp 1964-1965
This is all very confusing… Let’s turn to meta-analyses of RCTs for more clarity on the matter…
Thomson A. The enteral versus parenteral nutrition debate revisited. JPEN J. Parenter Enteral Nutr.2008; 32:474 -481
Is TPN really protective? Simpson F, Doig G. Parenteral vs enteral nutrition in the critically ill patient: a meta-analysis of trials using the intention to treat principle. Intensive Care Med. 2005;31(1):12-23
Is TPN really protective? Simpson F, Doig G. Parenteral vs enteral nutrition in the critically ill patient: a meta-analysis of trials using the intention to treat principle. Intensive Care Med. 2005;31(1):12-23
Thomson A. The enteral versus parenteral nutrition debate revisited. JPEN J. Parenter Enteral Nutr.2008; 32:474 -481
MORTALITY www.criticalcarenutrition.com
MORTALITY PN calories > EN calories www.criticalcarenutrition.com
MORTALITY PN calories = EN calories www.criticalcarenutrition.com
MORTALITY PN blood sugars > EN blood sugars www.criticalcarenutrition.com
INFECTIOUS COMPLICATIONS ARR = 0.17; NNT = 5.7 www.criticalcarenutrition.com
INFECTIONSPN calories > EN calories www.criticalcarenutrition.com
INFECTIONSPN calories = EN calories www.criticalcarenutrition.com
INFECTIONSPN blood sugars > EN blood sugars www.criticalcarenutrition.com
GUIDELINE CONCLUSIONS • The use of EN compared to PN is not associated with a reduction in mortality in critically ill patients. • The use of EN compared to PN is associated with a significant reduction in the number of infectious complications in the critically ill. • No difference found in ventilator days or LOS between groups receiving EN or PN. • Insufficient data to comment on other complications; hyperglycemia or higher calories not found to result in higher mortality of infections. • EN is associated with a cost savings when compared to PN. www.criticalcarenutrition.com
WHAT DOES THIS TELL ME? • Despite having clinical practice guidelines, route of nutrition is a topic that remains controversial. • As far as I can tell, the take home message should be: • Try to use EN if you can as it will decrease infectious complications, is cheaper, and will instantaneously give you another lumen. • Supplementing inadequate EN with PN has not been shown to be beneficial. • If you can’t use EN, PN is fine, though it may increase your rate of infections but not your LOS or mortality (this may only occur in patients that are overfed with PN however).
You decide to feed this patient enterally via an NG tube. You ask your resident about starting to feed the patient and he says, “you know he has had a really tough day, why don’t we wait until the morning to start his feeds”
Question #2 Does early enteral nutrition vs late enteral nutrition result in better outcomes in critically ill adult patients?(Noemie)
Why feed early? • Early EN improves wounds healing and host immune function • Decreases hypermetabolic response to tissue injury • Preserves intestinal mucosal integrity • Two meta-analysis recently published evalu Crit Care Med 2001;29(12):2264-2270
15 studies • All surgical patients • Early defined as < 36Hrs post admission or surgery Crit Care Med 2001;29(12):2264-2270
Mean Reduction in length of stay 2.2 days (CI 0.81-3.63) Crit Care Med 2001;29(12):2264-2270
Mortality in early 8 % vs 11.5% in delayed EN. Not statistically significant: RR 0.74 (0,37-1.48) Crit Care Med 2001;29(12):2264-2270
8 “level 2” RCTs • Defined early as within feeds started within 24-48hrs of admission • Only mechanically ventilated patients
Trend towards decrease mortality Heyland et al, JPEN, 2003; 27: 355-373
Trend toward decrease infectious complications • Final Recommendation: • Recommend early EN within 24-48H after admission to ICU Heyland et al, JPEN, 2003; 27: 355-373
Conclusion • Early EN is associated with a trend towards a reduction in mortality in critically ill patients. • Early EN is associated with a significant reduction in infectious complications • Early EN has no effect on ICU or hospital length of stay • Early EN improves nutritional intake. CriticalcareNutrition.com
Early aggressive vs early lower EN? CMAJ, 2004; 170 (2):197-204.
Intervention groups received more calories per day: 1264 Kcal vs 998 Kcal • Achieve 80% of goal feeds: 5.1 vs 4.8 days! • Significant shorter hospital stay • Trend toward decrease mortality CMAJ, 2004; 170 (2):197-204.
Conclusions: • May be associated with a reduction in mortality in the critically ill patient • May be associated with a reduction in hospital lengths of stay in the critically ill patient • Is associated with a trend towards a reduction in the # infections and complications in head injured patients. • Results in a significantly higher calorie intake/lower calorie deficit in head injured patients and other critically ill patients.
So the resident agrees to start feeding and now asks you how much do I order? • Question #3 Discuss the tools for estimating enteral feeding requirements in the critically ill adult patient. Please include a discussion of indirect calorimetry (TODD)
You initiate enteral feeding. A few hours later the nurse calls you to tell you that the patient gastric residuals are high. • Question #4 Does the use of a promotility agent impact patient outcome? ( please discuss some of the options for promotility agents) (SCOTT)
40-50% of critically ill patients experience some degree of slow gastric emptying • Increases risk of reflux and aspiration, as well as suboptimal nutrition. • Options are prokinetics (maxeran, erythromycin, naloxone, ?methylnaltrexone), postpyloric feeding, or TPN. • Regarding prokinetics little (if any) evidence exists regarding impact on “hard” outcomes.
Metoclopramide (maxeran), a dopamine antagonist has been shown to: • Improve gastric emptying in critically ill patients after a single dose. • Effect on the longer term success of feeding unknown.
Erythromycin (3mg/kg) has been shown to: • Increase gastric emptying. • Improve feeding success in previously feed intolerant patients.
Erythromycin vs. metoclopromide vs. both • Single double blind RCT (Nguyen, 2007) showed erythromycin 200 mg bid was more effective in reducing gastric residuals than maxeran 10 mg IV bid, but both treatments had rapid tachyphylaxis. • Combination rescue therapy was highly effective and had less tachyphylaxis. • A separate study confirmed that combination therapy was more effective than erythromycin alone in reducing gastric residuals. • Combination therapy has also been found to result in a significant higher calorie intake, lower gastric residual volumes and lower need for post pyloric feeds. • Concerns around routine erythromycin use include bacterial resistance, the potential for cardiac toxicity and tachyphylaxis.
Other outcomes • Multiple studies show benefit of promotility agents on overall nutritional intake. • In five studies of either maxeran or erythromycin used alone, no mortality benefit has been demonstrated. • In three studies looking at pneumonia or infection rates, only one (using naloxone), showed a significant reduction in pneumonia. The other two (using maxeran) showed no difference in pneumonia or infection rates.
Other outcomes - cont’d. • LOS, ventilator days - no differences have been shown in three studies that looked at these outcomes. • Conclusion: • 1) Motility agents have no effect on mortality or infectious complications in critically ill patients. • 2) Motility agents may be associated with an increase in gastric emptying, a reduction in feeding intolerance and a greater caloric intake in critically ill patients.
Recommendation • Based on 1 level 1 study and 5 level 2 studies, in critically ill patients who experience feed intolerance (high gastric residuals, emesis), we recommend the use of a promotility agent. Given the safety concerns associated with erythromycin, the recommendation is made for metoclopramide. • There are insufficient data to make a recommendation about the use of combined use of metoclopramide and erythromycin. • Other steps to reduce feeding intolerance and aspiration risk include head of bed elevation, control of pain and other contributing factors like hypotension and sepsis, avoidance of opiates.
Question #5 Are there other techniques to ensure adequate nutrition? Please discuss the utility of small bowel feeding, use of feeding protocols, body position. (NAISAN)