Download
1 / 69
840 likes | 1.93k Views
NUTRITION and IMMUNONUTRITION in the ICU. Marcia McDougall October 2007. ‘A slender and restricted diet is always dangerous in chronic and in acute diseases’. Hippocrates 400 B.C. Critical Illness. Heterogeneous patients Extreme physiological stress/organ failure

E N D
NUTRITION and IMMUNONUTRITION in the ICU Marcia McDougall October 2007
‘A slender and restricted diet is always dangerous in chronic and in acute diseases’ Hippocrates 400 B.C.
Critical Illness • Heterogeneous patients • Extreme physiological stress/organ failure • Acute phase response: TNF, IL-6, IL-1β • Immuno-suppression: monocytes, MØ, NK cells, T and B lymphocytes • Insulin resistance: hyperglycaemia • Protein loss and fat gain in muscle • Impaired gut function
Consequencesof malnutrition • Increased morbidity and mortality • Prolonged hospital stay • Impaired tissue function and wound healing • Defective muscle function, reduced respiratory and cardiac function • Immuno-suppression, increased risk of infection • CIPs lose around 2%/day muscle protein
Scale of the problem • McWhirter and Pennington 1994: • >40% of hospital patients malnourished on admission • Recent Scottish data 35% • Estimated cost to hospitals: £3.8bn/yr • Many ICU patients malnourished or at risk on ICU admission
ICU Nutrition through the ages Overfeeding 1980s
1970s: TPN - separate CH, AAs and Lipids • 2500-3000kcals/day: Lactic acidosis, high glucose loads, fatty livers, high insulin reqt • Single lumen C/Lines, no pumps • Urinary urea measured, N calculated • 1980s: Scientific studies of metabolism: recognition of overfeeding • 1990s: nitrogen limitation: 0.2g/kg/24hr, start of immunonutrition trials • 2000s: glucose control, specific nutrients
Nutrition trials in ICU • Small, underpowered • Heterogeneous and complex patients • Mixed nutritional status • Different feeding regimens • Underfeeding – failure to deliver nutrients • Overfeeding – adverse metabolic effects • Hyperglycaemia • Scientific basis essential
What is the evidence in ICU? • Early enteral feeding is best • Hyperglycaemia/overfeeding are bad • PN meta-analyses controversial • Nutritional deficit a/w worse outcome • EN a/w aspiration and VAP, PN infection • EN and PN can be used to achieve goals • Protocols improve delivery of feed • Some nutrients show promising results
Unanswered questions • Should we aim for full calorific delivery ASAP using EN + PN? • What are the best lipids to use in PN? • What is the role of small bowel feeding? • Are probiotics helpful? • Which patients will benefit from immuno-nutrition? • The future: targeted Nutrition Therapy?
Current practice - Scotland • SICS Nutrition Survey 2005-2006 • Wide variation in PN and NJ feeding use • Wide variation in opinions about nutrition • Lack of education about nutrition • Lack of interest from clinicians • Nutrition teams in 11/24 hospitals (QIS) • Discussion between dietitians and doctors limited
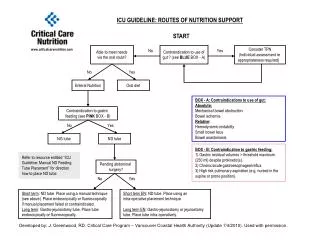
What is the maximum amount of time an ICU patient should go without nutrition?
Nutrition QI Study • Canadian Critical Care Network • 156 units cf CCCN guidelines • 8 Scotland, 22 UK • Adequacy of EN • Use of PN • Use of Immunonutrition • Protocols/Glycaemic control/Bed elevation
“systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances” U.S. Institute of Medicine “EBM - the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients” Sackett DL et al. BMJ 1996
What Guidelines are available? • Canadian Critical Care Network 2003/2007: Clinical Practice Guidelines • ICS: Practical Management of Parenteral Nutrition in Critically Ill Patients 2005 • ESPEN: Enteral Nutrition 2006 • NICE: Nutrition Support in Adults 2006
Organisation of Nutrition Support 3. NICE Guidelines for Nutrition Support in Adults 2006
Screen • Various nutritional screening tools • NRS 2002, SGA, MNA • Malnutrition Universal Screening Tool from the Malnutrition Advisory Group of BAPEN • Low risk: routine clinical care, • Medium risk: observe • High risk: treat- ‘refer to dietitian/local protocols’
Screening in ICU MUST not very helpful in guiding decisions • Almost all patients require artificial nutrition- cannot ‘observe’ • What about refeeding syndrome? • Needs adaptation using NICE Guidelines • Adapted MUST for ICU: Uses BMI/weight loss/food intake + refeeding risk assessment; linked to feeding flowchart
Step 3 Treat: Enteral if patient malnourished/at risk of malnutrition despite the use of oral interventions and has a functional and accessible gastrointestinal tract use the most appropriate route of access and mode of delivery 3. NICE Guidelines for Nutrition Support in Adults 2006
Step 3 Treat: PN if patient malnourished/at risk of malnutrition a non-functional, inaccessible or perforated gastrointestinal tract and has either inadequate or unsafe oral or enteral nutritional intake introduce progressively and monitor closely use the most appropriate route of access and mode of delivery 3. NICE Guidelines for Nutrition Support in Adults 2006
Routes Of feeding
REDUCED ENTERAL STIMULATION DECREASED: • Peyer’s patch leukotrienes + MAdCAM-1 • T & B cells in Peyer’s patches, Lamina propria & epithelium • Reduced secretory IgA and altered cytokines • Mucosal atrophy • Altered flora • Decreased gastric acid • Bacterial translocation
Enteral • Preserves intestinal mucosal structure and function • More physiological • Relatively non-invasive • Reduced risk of infectious complications cf PN (?) • Relatively cheap
NG problems • Risk of microaspiration in ICU • Risk of displacement • High gastric aspirates with opioids, sepsis, electrolyte imbalances • Reaching goals uncommon • PEG/gastrostomy feeding for long-term >4 weeks
Jejunal Feeding • Insertion • Surgical jejunostomy: at laparotomy • May reduce incidence of aspiration • Sometimes increases dose of EN given over NG • Indications
Parenteral Nutrition • GI tract not functional • GI tract cannot be accessed • Inadequate enteral nutrition <80% 3 days • Do not delay nutrition in malnourished • Keep 10ml/hr EN if possible
Supplemental PN • Optimize EN first if possible (??) • Villet: Clin Nutr 24, 2005: Caloric debt a/w increased LOS, vent days and complications • Need trial to compare early supplemental PN and early EN with early EN only • North America/Europe split over use of PN • Unanswered questions
How much to give in ICU? • Schofield equation/Harris Benedict e.g. for 65 year old woman: BMR = (9.2x weight in kg) + 687, = requirement in Kcal/24hr • Add Activity and Stress factors e.g. 10% for bedbound + 20-60% for sepsis/burns • For 65kg woman ventilated woman with sepsis: 1670 Kcal = approx 25 Kcal/kg/24hr • No dietitian? Rough guide: 25 Kcal/kg/day total energy. Increase to 30 as patient improves
How much to give? • 0.2g/Kg/day of Nitrogen (1.25g/kg/day protein) • 30 – 35ml fluid/kg/24 hours baseline • Add 2-2.5ml/kg/day of fluid for each degree of temperature • Account for excess fluid losses • Adequate electrolytes, micronutrients, vitamins • Avoid overfeeding • Obesity: feed to BMR, add stress factor only if severe i.e. burns/trauma
Refeeding Syndrome • Prisoners of war 1944-5, 1944: conscientious objectors in USA studied • Starvation: early use of glycogen stores for AAs - gluconeogenesis; 72 hrs: FFA oxidation; use of FFAs and ketones for energy source, low insulin • Atrophy of organs, reduced lean body mass
Refeeding syndrome • CH Feeding: shift to CH metabolism: insulin release • Stimulates PO42- and K+ shift into cells. PO42- drops lower (ATP, 2-3DPG). Mg2+ loss in urine 2o lowPO42-(Na+K+ATPase) • May get Lactic acidosis 2o conversion of pyruvate to lactate • Na+ and H2O shift out of cells – oedema; ECF expansion 2o reduced excretion of Na+ and H2O; • Hyperinsulinaemia is antinatriuretic • Protein synthesis increases cellr demand for PO42- and K+ • Thiamine deficiency occurs (co-factor in CH metabolism): encephalopathy
Refeeding Syndrome in ICU • Unlikely to be a clear diagnosis • Many deleterious effects: oedema, arrhythmias, pulmonary oedema, cardiac decompensation, respiratory weakness, fits, hypotension, leukocyte dysfunction, diarrhoea, coma, rhabdomyolysis, sudden death • Screen: nutritional history and electrolytes • Remember in HDU patients/malnourished ward patients • Poor awareness among doctors!
Risk of re-feeding syndrome Two or more of the following: • BMI less than 18.5 kg/m2 (<16) • unintentional weight loss greater than 10% within the last 3-6 months (>15%) • little or no nutritional intake for more than 5 days (>10) • Hx alcohol abuse or drugs including insulin, chemotherapy, antacids or diuretics • (Critically low levels of PO42-, K+ and Mg2+)
Managing refeeding problems • provide Thiamine/multivitamin/trace element supplementation • start nutrition support at 5-10 kcal/kg/day • increase levels slowly • restore circulatory volume • monitor fluid balance and clinical status • replace PO42-, K+ and Mg2+ • Reducefeeding rate if problems arise NICE Guidelines for Nutrition Support in Adults 2006
IMMUNONUTRITIONHuman Evolution • No ambulances/hospitals • First 72 hours after severe illness or injury crucial • Little hope of survival past this; not desirable • Significant stores of stress substrates not necessary e.g. glutamine
The Immune System A complex and interactive biological system that coordinates the detection, destruction and elimination of any foreign material or organism entering the body. • Oxidants: cytokines, NFkB, genes, inflamn • Nutrients: glutamine, FFAs, protein • Glutathione: oxidant defence • Anti-inflammatory molecules: attenuation
Critical Illness • Sepsis: Battle between inflammatory response and microbes/toxins • Trauma: SIRS to non-infectious insult • Minor insult: inflammatory response wins • Major insult: with support (antibiotics, fluids) body may be able to fight insult but in severe insult inflammatory response continues and causes organ damage, f/b immune paresis and 2° infection; death
THE ICU GAMBLEHow to tip the scales? LIFE DISABILITY Inflammation and resolution Inflammation, organ failure DEATH
Critical Illness • Small reductions in mortality over years • Increasing problems with infection • Advances in treatment have limited effects • Pathophysiology complex • The future: replacement of the body’s own ‘stress substrates’ • Could immunonutrition be the most important area in critical care development?
Failed ICU strategies • Anti-TNF antibodies • Steroids in sepsis – recent work suggests little effect • NO synthetase inhibitor: increased mortality • ??? Activated protein C - controversial
Immuno/Pharmaconutrition • ‘Disease-modulating’ nutrients • Attenuate metabolic response • Prevent oxidant stress • Favourably modulate immune response • Probiotics to alter gut environment • Glycaemic control: keep blood glucose <8mmol/l: reduces infections and organ failures
Glutamine • Non-essential amino acid – ‘conditionally essential’ in sepsis/major trauma • Vital to gut, immune cells, and kidney • Serves as metabolic fuel; precursor to DNA synthesis • BUT Levels drop after injury, exercise and stress. Very low in critical illness first 72 hours • Glutamine deficiency at onset of critical illness/sepsis correlated with increased mortality
Potential Beneficial Effects of Glutamine Enhanced Heat Shock Protein GLN Pool Enhanced insulin sensitivity Decreased Free Radical availability (Anti-inflammatory action) NF-kB ? Inflammatory Cytokine Attenuation Glutathione Synthesis Glutamine Therapy Reduced Translocation Enteric Bacteria or Endotoxins Maintenance of Intestinal Mucosal Barrier Fuel for Enterocytes Critical Illness Nuclotide Synthesis Preservation of TCA Function Reduction of Infectious complications Maintenance of Lymphocyte Function Fuel for Lymphocytes Anti-catabolic effect Preserved Cellular Energetics- ATP content Preservation of Muscle mass GLN pool Wischmeyer PE, Curr Opin Clin Nutr Metab Care 6: 217-222, 2003
Glutamine trials • Modest reduction in mortality/infections in 9 studies of glutamine-supplemented PN • Improvement in morbidity and mortality in 2 studies of enteral glutamine in burns and trauma patients • CCCN recommend enteral glutamine for burns and trauma and IV glutamine to be given with parenteral nutrition • SIGNET and REDOXs awaited