Download
1 / 82
950 likes | 1.82k Views
DIAGNOSIS AND TREATMENT OF HERPES SIMPLEX KERATITIS UPDATE. XVI JORNADAS DE OFTALMOLOGIA DR. BENJAMIN BOYD AUGUST, 2005. RICHARD L. ABBOTT, M.D. PROFESSOR OF OPHTHALMOLOGY. RICHARD L. UCSF FRANCIS I. PROCTOR FOUNDATION. HUMANS ARE THE . HUMANS ARE THE ONLY NATURAL RESERVOIR OF HSV.

E N D
DIAGNOSIS AND TREATMENT OF HERPES SIMPLEX KERATITIS UPDATE XVI JORNADAS DE OFTALMOLOGIA DR. BENJAMIN BOYD AUGUST, 2005
RICHARD L. ABBOTT, M.D. PROFESSOR OF OPHTHALMOLOGY RICHARD L. UCSF FRANCIS I. PROCTOR FOUNDATION
HUMANS ARE THE HUMANS ARE THE ONLY NATURAL RESERVOIR OF HSV HSV 1 OROPHARYNX HSV 2 GENITAL AREA
TRIFLURIDINE VIDARABINE IDOXURIDINE
HSV OCULAR DISEASE • Approx. 1/2 million people in U.S. • Approx. 20-45% of world population • Approx. 50,000 active episodes annually • Approx. 20,000 new cases annually • By age 5….60% of population infected • Only 6% develop clinical manifestations
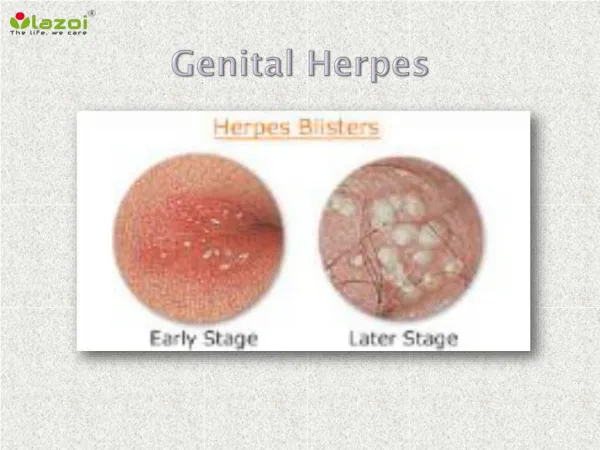
PRIMARY HERPES SIMPLEX • Acquired from environment (oral lesions, saliva) • Not from viral latency • Unilateral vesicular blepharoconjuntivitis • Pruritic vessicles of lids, skin, eyelid margin • Follicular conjunctivitis • Palpable preauricular lymph node • PEK (RARE dendrite)
INFECTIOUS EPITHELIAL KERATITIS • Corneal vessicles (PEK) • Dendrite • Geographic (Amoeboid) ulcers • Marginal ulcers (Limbal KC) • May be associated with conjunctivitis
TREATMENTPrimary Herpes Simplex • Oral Acyclovir • Topical Trifluridine • Observation (self-limited)
TYPICAL CORNEAL DENDRITE • Of first importance in making the clinical diagnosis • Dendron (Greek- “Tree”) • True ulcer – extends through BM
DDX:DENDRITIC KERATITIS • HSV • HZV • Healing epithelium • Thimerosal (Toxicity) • SCL
GEOGRAPHIC (AMOEBOID) ULCER • “Wide” dendrite • DDX epithelial defect – scalloped border • 4-20% of initial lesions • +/-Associated with previous steroid use
LIMBAL (MARGINAL) HSV-I KERATITIS • Atypical presentation • More resistant to Rx • DDX: Staph marginal infiltrate • No epithelial defect • Progress circumferential • Associated with blepharitis • Typical location 2, 4, 8, 10
INCREASED INFLAMMATION WBC INFILTRATION
Goal: Purpose: Diagnosis: Eliminate virus in short time Decrease potential risk for immune-mediated disease Decrease structural damage Clinical, culture, PCR TREATMENTInfectious Epithelial Keratitis
TREATMENTInfectious Epithelial Keratitis • Gentle debridement • Topical antivirals (10-14 days max) • Viroptic 1% q 2h or • Vira A 5X/day • If no response 72 hours – STOP • Resistance rate - 3%
TREATMENTInfectious Epithelial Keratitis • If slow healing, consider toxicity • If epith ulcer persists, consider neurotrophic • Avoid steroids
ACYCLOVIR REGIMEN • 400 mg 5x/day for 10-14 days • Reduce to b.i.d. for 10 days • Very safe • Headaches, GI upset • Watch dose renal disease
HSV IRIDOCYCLITIS • 1-9% of all non-traumatic anterior uveitis • May occur independently • Live virus in aqueous • Average time to resolution: 4 weeks • Treat with topical steroids, cycloplegics, and PO Acyclovir • Watch IOP – Trabeculitis
SECTOR IRIS ATROPHY • See in both Simplex and Zoster • Older patient - probably Zoster • If in doubt - treat with Zoster doses
STROMAL KERATITIS • 2% of initial episodes • 20-48% of recurrent HSV • Disciform (Immune only) • Necrotizing (direct viral invasion) • Metaherpetic (post-herpetic trophic ulcer)
IMMUNE (INTERSTITIAL) STROMAL KERATITIS (DISCIFORM) • Cell mediated immune response to viral antigens in stroma or endothelium
DISCIFORM KERATITIS • +/- Previous HSV epithelial keratitis • Non-necrotizing • Focal, multifocal, or diffuse area of edema • Mild lymphocytic stromal inflammatory infiltrate- chronic and recurrent • Epithelium intact • Descemet’s folds and KP
DISCIFORM KERATITIS • Differential diagnosis • HSV • HZV • Vaccinia • Mumps • Varicella
STROMAL DISEASE • Treatment goals • Eradicate HSV • Limit scarring • Limit lipid deposition
TREATMENTStromal Keratitis • Treatment depends on severity and location of inflammation • Necrotizing keratitis • Interstitial keratitis • Immune rings • Limbal vasculitis • Disciform keratitis
TREATMENTDisciform Keratitis • Conservative - self limited • Oral Acyclovir 400mg 5x/day • Topical steroid - rapid taper • No topical antiviral (poor penetration)
NECROTIZING STROMAL KERATITIS • WBC’s (dense infiltrate with overlying defect • Blood vessels • Thinning • Scarring • Necrosis and perforation