Download
1 / 34
340 likes | 578 Views
Gastrointestinal Bleeding. Group D. Case Illustration. Name : Mr. D Age : 33 years old Religion : Moslem Marital status : single Address : Jl. Cilamaya , Cikarang Village , East Krawang Occupation : jobless Education level : elementary school

E N D
Gastrointestinal Bleeding Group D
Case Illustration • Name : Mr. D • Age : 33 years old • Religion : Moslem • Marital status : single • Address : Jl. Cilamaya, Cikarang Village, East Krawang • Occupation : jobless • Education level : elementary school • Med. Record : 341.96.59
History of Present Illness • Chief complaint • Vomiting blood since 3 days prior hospitalization • HPI: • 2 weeks before hospitalization, the patient vomiting blood which was dark in colour for 2-3 times per day. The amount of blood coming out was about 10 cc each time. The patient also admits the presence of nausea and sharp pain in the upper part of the stomach. The pain did not spreading to his back and occurs intermittently. The pain on the stomach also wasn’t relieved by food or but by consuming Mylanta, bloating (+), easy satiety (+). Furthermore, the patient also complaints of fever which occurs intermittently but the temperature were not very high. He also has cough and his voice became harsh. However, there was no sputum at all. He also complaints fatigue, chilling, and muscle ache.
3 days prior hospital admission, the complaints was worsening. The patient vomit 2-3 times per day more blood came out. Approximately 100 cc was expelled each time he vomits. The presence of upper stomach pain, nausea, vomit, and loss of appetite was admitted. • The patient had history of drinking alcohol but he never had history of traditional medicine consumption, drugs usage of any kind especially, blood transfusion, or liver disease. He knew that he has hypertension 10 years ago but never control nor get medication for it. • He denies history of icteric skin, light stool, dark urine, ascites, edema, or hepar disease. • He denies the presence of diabetes mellitus, asthma, allergy, and heart or lung disease.
History of Past Illness • There was no similar complaint like this before • Family History of Illness • The patient denies any presence of diabetes mellitus, hypertension, asthma, allergy, heart or lung disease. No other families have similira complaint. • History of Occupation, Social-Economy and Habit • The patient work as a “pemulung” and homeless • He never married • He has smoking habit and used to consume 2 packs of cigarettes per day
Physical Examination • Status Generalis • Consciousness : Compos mentis • Blood Pressure : 130/90 mmHg • Heart Rate : 96x/min • Temperature : 37oC • Respiratory Rate : 20x/min • Body Height : 165 cm • Body Weight : 50 kg
Head • Normocephal, no deformity. • Hair • Black, not easy to be pulled off. • Eye • Pale conjunctiva -/-, icteric sclera -/-, round pupil with diameter 3 mm/3mm, direct light reflex +/+, indirect light reflex +/+ • Ear • No deformity, no edema, cerument +/+ minimal, secrete -/-, light reflex +/+, intact tympanic membrane
Nose • No deformity, no septum deviation, no hypertrophy conchae, no secrete • Throat • Uvula located in the middle, no hyperemic pharynx, tonsil T1-T1 • Teeth and Mouth • Humid mucosa, caries dentis (+) • Neck • Trachea located in the middle, JVP 5-2 cm H2O, thyroid not palpable, lymph node not palpable
Lung • I: There is a tattoo on his chest, symmetric in static and dynamic condition • P: Fremitus left = right • P: sonor on all lung fields • A: vesicular/vesicular, wheezing -/-, ronchi +/+ • Heart • Ictus cordis was not seen and not palpable, right heart border on ICS 4 right midsternal line, left heart border on ICS 5 left midclavicular line, S1S2 normal, no murmur, no gallop. • Abdomen • supple, pressure pain (+) epigastrium, hepar was palpable 2 fingers below processus xyphoideus, lien was not palpable, tympanic on all abdomen fileds, bowel sound (+) normal.
Extremity • Warm acral, CRT < 3”, edema (+/-), paresis (-), Palmar erythema (-), flapping tremor (-), tattoo (+). • Anal • rectal tousche: adequate sphincter power, the ampulla was not collapse, smooth mucosa, faeces (+) no blood.
AFB (16/12/10): Negative • Thorax roentgen: CTR < 50%, infiltrate +/+ • ECG: Sinus rythem, QRS rate 100x/min, PR int < 0.2, QRS int <0.12, ST-T change (-), Inverted T (-), LVH (-), RVH (-), LBBB (-), RBBB (-).
List of Problem • Acute on CKD dd/ CKD dd/ AKI • Community Acquired Pneumonia • Hypertension grade I • Anemia • PT and APTT elongation • Hematemesis • Hematuria • Dyspepsia
Analysis • Acute on CKD • Anamnesis • History of hypertension for more than 10 years, nausea, and vomiting. Two weeks before hospitalization, the patient vomit blood which was worsening since 3 days prior hospitalization. No complaints on urination, no dyspneu, no edema. • PE • BP: 130/90 mmHg • Eye: Anemic conjunctiva +/+, Icteric sclera -/- • Mouth: dry blood on the mucosa • Neck: JVP 5-2cmH2O • Lung: ronchi +/+ • Ext: edema +/-
Diagnosis • Acute on CKD with anemia and acidosis metabolic dd/ CKD stage V • Plan • Renal USG, measure CCT, Ca, Ur/Cr, Blood gas analysis, electrolyte serial, lipid profile and uric acid • Treatment • Bed rest • Renal diet 1900 kcal/ day, protein 0.8 g/kgBB/day, liquid diet 4x100cc • Fluid balance per 24 hour • AF 1x3 • Bic nat 3x2 • CaCO3 3x1 • B12 3x1
Community Acquired Pneumonia • Anamnesis • Cough (+) without sputum, fever (+) • PE • Rh +/+, CXR: infiltrate +/+ • Diagnosis • CAP dd/ lung TB • Plan • Sputum culture, AFB 3x, MDR, resistant test • Treatment • O2 3L/mint • Flumucyl 3xCI • Cefotaxime 2x1 g • Azithromycin 1x500 mg
Hypertension grade I • Anamnesis • History of hypertension (+) not controlled • PE • BP: 130/90 • Cardiomegaly (-) • ECG: LVH (-), RVH (-), BBB (-), inverted T (-), • Roentgen: CTR < 50% • Diagnosis • Hypertension grade I • Plan • Echocardiography, ECG, Renal USG, Ur/Cr, urinalysis • Treatment • Renal diet 1900 kcal/day through NGT 4x100 cc • Amlodipin 1x10 mg
Anemia • Anamnesis • History of hematemesis melena, hypertension (+), renal disease (-) • PE • Eye: Anemic conjucntiva +/+ • Neck: JVP 5-2cmH2O • Heart: S1S2 normal, murmur (-), gallop (-) • Abdomen: Hepar was palpable 2 fingers below processus xyphoideus • Ext: edema (-) • Lab: Hb=6.7, MCV=84 • Diagnosis • Anemia microcytic normochromic • Plan • Gamma GT, reticulocyte, Fe TIBC, Ferritin • Treatment • Blood transfusion if needed with target Hb=10g/dL
PT and APTT elongation • Anamnesis • History of yellowish (+), alcohol consumption (+) • PE • Hepar was palpable 2 fingers below processus xyphoideus • PT/APTT=2.3/2.5 • Diagnosis • PT/APTT elongation e.c DIC dd/CLD • Plan • PT/APTT, Hb, d-dimer • Treatment • Vitamin 3x1 • FFP transfusion
Hematemesis • Anamnesis • 2 weeks of hematemesis, 3 days of hematemesis melena • PE • Eye: Anemic conjunctiva +/+, icteric sclera -/- • Lung: rh +/+ • Heart: S1S2 normal, murmur (-), gallop (-) • Abdomen: hepar was palpable 2 fingers below processus xyphoideus • Hb=6.8, PT/APTT=16.5/56.7, Thr=340000 • Diagnosis • Hematemesis e.c peptic ulcer dd/ PVO dd/ gastritis erosiva
Plan • EGD, USG abdomen, SGOT/SGPT, Albumin, Globulin, CHC, blood smear • Treatment • Observation • Sucralfat 3x1 • Domperidone 3x10 • Vit K 3x1 • Transamin 3x1 • Omeprazole 1x1 20mg
Hematuria • Anamnesis • Pain during urination (-), fever (+), waist pain (-) • PE • CVA -/- • Urinalysis: blood (+), Erythrocyte=15-16 • Diagnosis • Hematuria microscopic e.c. catheter trauma • Plan • Repeat urinalysis • Treatment
Dyspepsia • Anamnesis • Nausea (+), vomiting (+) • PE • Epigastric pressure pain (+) • Diagnosis • Dyspeptic syndrome • Plan • - • Treatment • Omeprazole 1x40 mg • Domperidone 3x10 mg
Prognosis • Quo ad vitam : dubia ad malam • Quo ad functionam : dubia ad malam • Quo ad sanationam : dubia ad malam
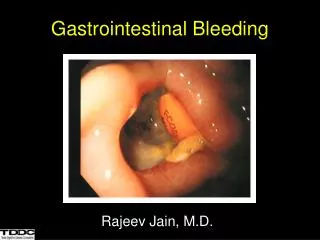
Discussion • From the case we know patient experienced black blood vomit. • It means the blood coming out has already been oxidized by gastric acid. • Patient also complaints about black stool, which means the feces has already for 14 hours in GI track.
Clinically upper GI track bleeding is divided into varices and non-varices bleeding. • So we need to find if there are any symptoms and sign of liver disease such as nausea, vomit, fatigue, icteric skin, light stool, dark urine, ascites, edema, epigastrium discomfort, caput medusa, erythema Palmaris. • From anamnesis all those symptoms and signs were denied, but liver was enlarged. • From the SGOT/SGPT results show the increase the marker but it decrease at the next examination.
From the history there are was history of alcohol, but no anti-coagulant and NSAIDs consumption. • Infection H.pylori need to be excluded by Urea Breath Test since H.pylori produce urease. • But in this patient the test is not done. So we can conclude it is possibly peptic ulcer. • We can exclude the Mallory weiss syndrome since the blood vomiting is occurred without any previous vomiting, coughing, and retching. • the other possibility is erosive gastritis.
There types of peptic ulcer classification according Johnson Classification: • Type I: Ulcer along the body of the stomach, most often along the lesser curve at incisuraangularis along the locus minorisresistentiae. • Type II: Ulcer in the body in combination with duodenal ulcers. Associated with acid oversecretion. • Type III: In the pyloric channel within 3 cm of pylorus. Associated with acid oversecretion. • Type IV: Proximal gastroesophageal ulcer • Type V: Can occur throughout the stomach. Associated with chronic NSAID and ASA use.
The associated risk factors with UGIB in patients with peptic ulcer were: age lower than 60 years; smoking; history of UGIB; and alcohol consumption. • Upper endoscopy is the best of choice in patients with UGIB and should be performed urgently in patients with hemodynamic instability (hypotension, tachycardia, or postural changes in heart rate or blood pressure). • Early endoscopy is also beneficial in cases of milder bleeding for management decisions.
Therapy method with endoscopy aims to active or visible peptic ulcer, consist of contact thermal, non-contact thermal, and nonthermal. • Endoscopic therapy could be applied to 90% of cases. The other 10% because of technical problem, such as massive bleeding and site of bleeding is unreachable. • Peptic ulcer bleeding can resolve spontaneously in 80% cases, but only 30% arterial bleeding can resolve spontaneously. • The simplest endocopy therapy is injection of adreanaline 1:10.000 in 0.5-1 mL, maximal doses 10 mL. Success rate of therapy can reach 95%.