Download
1 / 47
520 likes | 1.1k Views
Gastrointestinal Bleeding. Amr Mohsen, M.D., FRCS(Ed) Professor of Surgery, Cairo University. Gastrointestinal Bleeding Spectrum of Disease. NOT one disease but various pathological processes Common problem Mortality rate still 10% Massive acute hemorrhage to occult, trivial

E N D
Gastrointestinal Bleeding Amr Mohsen, M.D., FRCS(Ed) Professor of Surgery, Cairo University
Gastrointestinal BleedingSpectrum of Disease • NOT one disease but various pathological processes • Common problem • Mortality rate still 10% • Massive acute hemorrhage to occult, trivial • Timely evaluation is critical to proper management
Gastrointestinal BleedingDefinition of Terms • Upper Gastrointestinal Bleeding: proximal to Ligament of Treitz • Lower Gastrointestinal Bleeding: distal to the ligament of Treitz • Hematemesis: vomiting of blood • Melena: Passage of black tarry stools • Hematochezia: Passage of fresh blood per rectum
Gastrointestinal BleedingDefinition of Terms • Manifest bleeding • Occult bleeding • Bleeding of obscure origin
I Chronic Gastrointestinal BleedingOccult Bleeding – Manifestations • Weakness • Fatigue • Shortness of breath • Faintness • Accidentally discovered anemia • Routine screening
I Chronic Gastrointestinal BleedingOccult Bleeding – Causes - Diagnosis • GIT malignancy • GERD & esophagitis • Peptic ulcer • NSAIDs • GIT polyps Detection depends on peroxidase activity of hemoglobin Guaiac test Hemoccult test
IIAcute Gastrointestinal BleedingInitial Evaluation • Estimate severity of bleeding • Institute resuscitation • Localize site of bleeding (UGI vs LGI) • Diagnose and treat specific lesion
II Acute Gastrointestinal BleedingEstimation of Severity BEST METHOD: vital signs • Massive hemorrhage: shock (supine hypotension) 20-25% loss of vascular volume • Submassive hemorrhage: orthostatic hypotension 15-20% loss of vascular volume • Trivial hemorrhage: No change in vital signs < 15% loss of vascular volume
II Acute Gastrointestinal BleedingLocalization • Distinguishing LGI and UGI • Clincal Signs • Hematemesis: UGI bleeding • Melena: Usually UGI • Hematochezia: Usually LGI • Nasogastric aspirate (ALL PATIENTS) • Lavage +: UGI bleeding • 15% miss rate
IIa Acute UGI BleedingManagement • Hematemesis, or melena is an emergency. • Admission to an ICU for all patients with severe GI bleeding. • The team approach includes a gastroenterologist, a surgeon with expertise in GI surgery, and skilled nurses. • A major cause of morbidity and mortality is aspiration of blood. To prevent this complication in patients with altered mental status, endotracheal intubation should be considered.
IIa Acute Gastrointestinal BleedingResuscitation • All patients need 2 large-bore IVs • Crystalloid solutions until blood available • Send blood for Hct, coagulation studies (PT, PTT, platelet), crossmatch • Transfuse blood for: • Obvious massive blood loss • Hematocrit < 25% with active bleeding • Symtpoms due to low Hct • Correct coagulopathies • Fresh frozen plasma • Platelet transfusion
IIa Acute UGI BleedingEtiology (Egypt) • Esophageal varices 55% • Acute gastric erosions 15% • Chronic DU • Chronic GU • Esphagitis & erosions • Mallory Weiss tears • Duodenitis • Gastric cancer • Coagulopathies
IIa Acute UGI BleedingDiagnosis • History • of previous bleeding • of peptic ulcer symptoms • of previous surgery • of medications: NSAID • Physical Exam • Stigmata of cirrhosis: spider angiomata, jaundice, gynecomastia, palmar erythema, testicular atropy, splenomegaly, ascites, noular liver. • Surgical scars • Tenderness
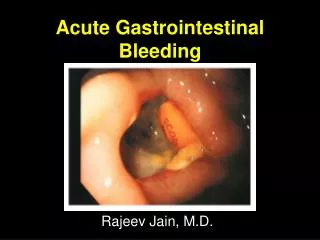
IIa Acute UGI BleedingDiagnostic Procedures • Endoscopy • 90-95% accurate • Diagnosis and treatment • Barium radiography • 80% accurate • Barium makes further studies difficult • Arteriography (failure of localization / active bleeding) • Nuclear Scanning (Technetium-99m) ?? Endoscopy is routinely used first, particularly in patients with significant hemorrhage
IIa Acute UGI BleedingEndoscopy Varices Normal
IIa Acute UGI BleedingEndoscopy Acute gastric erosions Signs of recent bleeding
IIa Acute UGI BleedingEndoscopy DU – signs of recent bleeding
IIa Acute UGI BleedingEndoscopy GU Blood clot Visible vessel
IIa Acute UGI BleedingEndoscopy Mallory Weiss tear
IIa Acute UGI BleedingTreatment of Specific Lesions Esophageal varices URGENT • Endoscopic sclerotherapy or banding • Vasopressin infusion • Surgery
IIa Acute UGI BleedingTreatment of Specific Lesions Esophageal varices Sengstaken tube Temporary measure
IIa Acute UGI BleedingTreatment of Specific Lesions Esophageal varices • Endoscopic sclerotherapy or banding
IIa Acute UGI BleedingTreatment of Specific Lesions Esophageal varices • Endoscopic sclerotherapy or banding • Highly successful • Failure Repeat injection • Followed by chronic sclerotherapy • Failure rate ~15% From esophageal varices Missing fundal varices Difficulty injecting fundal varices
IIa Acute UGI BleedingTreatment of Specific Lesions Esophageal varices 2. Vasopressin (1 unit/min) IV infusion Beware of coronary heart disease
IIa Acute UGI BleedingTreatment of Specific Lesions Esophageal varices 3. Urgent surgery Emergency shunt surgery is losing favor
IIa Acute UGI BleedingTreatment of Specific Lesions Esophageal varices 3. Urgent surgery Most popular procedure
IIa Acute UGI BleedingTreatment of Specific Lesions Peptic Ulcers • Antacids or H2 blockers and proton pump antagonists promote healing but DON’T stop acute bleeding URGENT • Endoscopic coagulation • Angiographic embolization • Surgery
IIa Acute UGI BleedingTreatment of Specific Lesions Peptic Ulcers Surgery
IIb Acute LGI BleedingGeneral Considerations • Spontaneous remission rate is 80% Bleeding has usually ceased by the time the patient presents to hospital • No source of bleeding can be identified in 12% • Bleeding is recurrent in 25%
IIb Acute LGI BleedingCommon causes • Hemorrhoidal bleeding • Fresh bright red • Jet or drops separate from stools • With straining at end of defecation • Massive bleeding in adults 1. Diverticula 2. UC 3. Ischemic colitis 4. Angiodysplasia 5. Massive bleeding from upper GIT • Massive bleeding in children Meckel’s diverticulum
IIb Acute LGI BleedingGeneral Considerations • Initial evaluation is the same • Judge severity • Resuscitate • Localize site (usually difficult) • Patient usually notes hematochezia (bright red rectal bleeding) • Most of LGI bleeding is from anus or rectum especially trivial bleeding
IIb Acute LGI BleedingManagement • Hematochezia should be considered an emergency. • Admission to an ICU is recommended for all patients with severe GI bleeding. • The team approach includes a gastroenterologist, a surgeon with expertise in GI surgery, and skilled nurses.
IIb Acute LGI BleedingDiagnosis • History • Previous bleeding episodes • Rectal pain/hemorrhoids • IBD • Change in stool caliber • Weight loss • Physical Exam • Rectal examination: hemorrhoids, tears, fissures, fistulas • Anoscopy: hemorroids, fissures • Sigmoidoscopy
IIb Acute LGI BleedingEvaluation • Nasogastric tube if massive bleeding • Sigmoidoscopy • Colonoscopy • Angiography require blood loss > 0.5 ml/min • Isotope scanning • Barium enema not for initial diagnosis
IIb Acute LGI BleedingEvaluation Angiodysplasia (usually Rt colon)
IIb Acute LGI BleedingEvaluation Diverticula (usually Lt colon)
IIb Acute LGI BleedingEvaluation Normal colon UC
IIb Acute LGI BleedingEvaluation Ischemic colitis (usually splenic flexure)
IIb Acute LGI BleedingEvaluation Diverticula (usually Lt colon)
IIb Acute LGI BleedingManagement 1. 80% of bleeding cases stop spontaneously 2. Arteriography & embolization Angiodyaplasia Argon beam coagulation 3. Urgent surgery Preoperative localization Resection No localization + I.O. colonoscopy High failure After treatment and follow-up
III Bleeding of obscure originDefinition the cause of the bleeding has not been determined after an initial gastrointestinal evaluation May be occult or manifest
III Bleeding of obscure originSources In 38% of patients the source of bleeding is located in the distal duodenum and proximal jejunum Duodeno-jejunal arteriovenous malformations (AVMs) are the most common cause for bleeding
III Bleeding of obscure originManagement steps • Repeat upper and/or lower GI endoscopy • Enteroscopy • Push enteroscopy. can be advanced as much as 100 cm past the ligament of Treitz • Sonde enteroscopy, a tube is advanced by peristalsis into the small intestine. Lengthy and uncomfortable • Swallowed capsule endoscopy
III Bleeding of obscure originManagement steps • Isotope-labelled RBCs scan (0.1-0.4ml/min) • Mesenteric angiography (>0.5ml/min) • Meckel’s scan • Barium meal for chronic cases (limited value in AVM) • intraoperative enteroscopy
Application • Case variation • Surgeon’s experience • Hospital facilities Individualize management Don’t hesitate to TRANSFER