Download
1 / 28
310 likes | 837 Views
Regaining Postural Stability and Balance. Rehabilitation Techniques for Sports Medicine and Athletic Training William E. Prentice. Introduction.

E N D
Regaining Postural Stability and Balance Rehabilitation Techniques for Sports Medicine and Athletic Training William E. Prentice
Introduction • Muscular weakness, proprioceptive deficits, and range of motion deficits may challenge a persons ability to maintain their center of gravity (COG) • May lead to loss of balance • Balance is the single most important element dictating movement strategies • Dynamic process involving multiple neurological pathways
Introduction • Joint position sense , proprioception, and kinesthesia are vital to all athletic performance requiring balance • Ability to balance and maintain postural stability is essential to an athlete who is acquiring or reacquiring complex motor skills
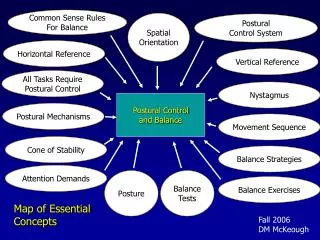
Postural control system • Complex process involving sensory and motor components • Most daily activities such as, walking, climbing stairs, throwing a ball, require static foot placement with controlled balance shifts • Balance should be considered both a static and dynamic process
Postural control system • Impaired balance is a result of one or a combination of two reasons • Position of COG relative to base of support is not accurately sensed • Automatic movements required to bring COG to a balanced position are not timely or effectively coordinated
Postural control system • Position of the body in relation to gravity and its surroundings is sensed by combining visual, vestibular and somatosensory (proprioceptive)inputs • Balanced movements also involve motions of the ankle, knee, and hip joints • Primary mechanisms for controlling balance occur in joints of the lower extremity • Postural control system operates as a feedback control circuit between brain and the musculoskeletal system
Somatosensory input • Mechanoreceptors transmit messages to brain through sensory nerves in spinal cord • Helps to control proprioception or body/joint position • Provides information concerning the orientation of body parts to one another and to the support surface
Balance & Closed Kinetic Chain • Balance is the process of maintaining the COG within the body's base of support • Within kinetic chain each moving segment transmits forces to every other segment along chain • Maintaining equilibrium or balance is associated with injuries along the closed kinetic chain • Injuries to any one of the joints or corresponding muscles along kinetic chain can result in loss of appropriate feedback for maintaining balance
Control of Balance • Human body is a tall structure on a relatively small base • COG is quite high, just above pelvis • Somatosensory input is preferred sense for balance • i.e. : feet in contact with support surface and detection of joint movement
Control of Balance • Visual input • Measures orientation of the eyes and head in relation to surrounding objects • If eyes are closed balance becomes more difficult • Vestibular input • Sensory system that is leading contributor to response to movement and sense of balance • Sends signals, primarily to neural structures that control our eye movement, and to muscles that keep us upright
Proprioception & Kinesthesia • Proprioception: ability to determine the position of a joint in space • Kinesthesia: ability to detect movement • Mediated by mechanoreceptors found in muscle and joints and by cutaneous, visual and vestibular input
Proprioception & Kinesthesia • Joint mechanoreceptors • Found in ligaments, capsules, menisci, labra and fat pads • Sensitive to change in shape of joint structures and rate and direction of movement of joint • Most active at end ranges of motion
Proprioception & Kinesthesia • Muscle mechanoreceptors • Found in muscles and tendons • Muscle spindles and Golgi Tendon Organs • Muscle spindles sensitive to changes in length of muscle • Golgi tendon organs sensitive to changes in tension
Assessment of Balance • Subjective Assessments: Romberg's & Balance Error Scoring System (BESS) • Romberg's test • Feet together, arms out to side, and eyes closed • Positive test: sway or fall to one side • indicates loss of proprioception
Assessment of Balance • Balance Error Scoring System (BESS) • 3 stances: double , single, and tandem • Completed 2 x each: Once on firm surface and once on unstable surface (Foam pad) • Total of 6 trials • Hands on iliac crest and eyes closed • In SL ex. Non stance leg held at 20-30 degrees hip flexion and 40 to 50 degrees of knee flexion
Assessment of Balance BESS Assessment Continued • 20 second test begins when eyes close • Single leg stance on non-dominant leg (NDL) and NDL is in the rear for tandem stance • Upon losing balance athlete returns to testing position as quickly as possible
Assessment of Balance • Balance Error Scoring System (BESS) • Scoring • 1 point added for each error that occurs • Hands lifted off iliac crest • Opening eyes • Step, stumble or fall • Moving hip into > 30 degrees of flexion or Abduction • Lifting forefoot or heel • Remaining out of testing position >5 seconds • Higher scores represent poor balance
Assessment of Balance • Dynamic balance test include functional reach test, timed agility, figure 8’s, carioca, or hop test • Ability to maintain upright posture while moving
Assessment of Balance • Advancements in technology have provided equipment to quantitatively assess and train dynamic balance • Mostly computer -interfaced force- plate technology • Potential to assess possible abnormalities that might be associated with injury and help create appropriate training programs
Injury & Balance • Stretched or damaged ligaments may fail to provide adequate neural feedback • May contribute to decreased proprioceptive mechanisms, and thus decreased balance • Increased postural sway and balance instability contributed to neurological factors and biomechanical factors after injury
Balance Training • Rehab program, especially for lower extremities must include exercises to improve balance and postural equilibrium • Any injury can cause disruption at some point between COG and base of support • If neglected can lead to reinjury, decreased performance, or other injuries
Balance Training • 5 general rules • Safe, yet challenging • Stress multiple planes of motion • Incorporate multisensory approach • Begin with static, bilateral stable surface and progress to dynamic, unilateral, and unstable surface • Progress toward sport specific activity
Balance Training • Balance Exercises • Static: COG maintained over fixed base of support while on stable surface • Semi-dynamic: • Maintain COG over fixed base on moving support or unstable surface • Person transfers their COG over a fixed base of support on stable surface through range and/or directions
Balance Training • Balance Exercises • Dynamic: maintenance of COG over moving base of support • Usually stable surface, but could be unstable • Base of support always changing position so COG is forced adjust with each movement • Functional • Same as dynamic, but add sport specific tasks
Balance Training • Phase I • Can be initiated once athlete can bear weight on the extremity • Static, non ballistic exercise • Hard firm surface • Bilateral to unilateral (double leg to single leg) • Eyes opened to eyes closed • Progress to unstable surface, perturbations (tapsor movement) • Overload or stress somatosensory system
Balance Training • Phase II • Transition of static to semi-dynamic & dynamic ex. • Important for running, jumping, and cutting athletes • Progress only if sufficient healing has occurred and ROM, muscle strength and endurance is adequate • Balance through movement • Controlled hip and knee flexion and smooth return to stabilization position • Progress to added resistance and more difficult movement patterns
Balance Training • Phase III • Dynamic & Functional exercises • Slow speed to fast speed • Low force to high force • Controlled to uncontrolled activities • Jumping or hopping activities • Bilateral to unilateral • Single plane to multi-plane • Exercises may differ between athletes • Be sport specific
Conclusion • Balance and postural stability critical to athletic performance and injury prevention • A rehabilitation program must include functional exercises that incorporate balance and proprioceptive training • Prepare athlete for return to activity • Failure address balance problems may predispose athlete to reinjury and injury • Use imagination, be creative • Use sport specific tasks