Download
1 / 1
10 likes | 141 Views
Perceived Emotional Intelligence and Health Kyle S. Page, Sue C. Jacobs, Claudia Porras, and Michele Pettit Oklahoma State University. PEARSON CORRELATIONS TMMS-A TMMS-C TMMS-R BSCI-SU BSCI-D BSCI-E BSCI-PL TMMS-A 1 TMMS-C .287** 1

E N D
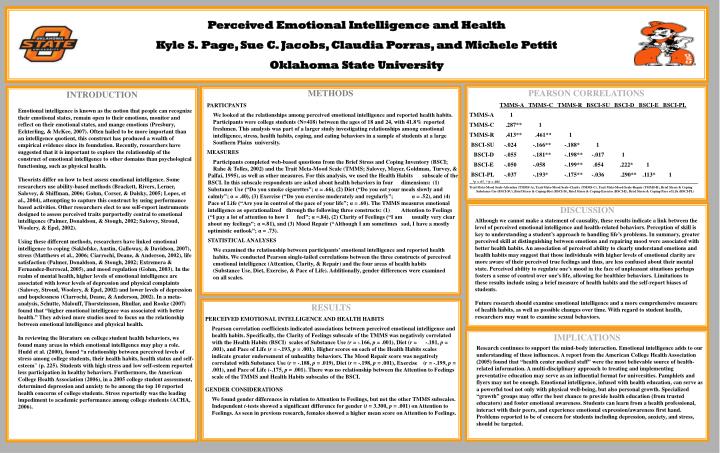
Perceived Emotional Intelligence and Health Kyle S.Page, Sue C. Jacobs, Claudia Porras, and Michele Pettit Oklahoma State University PEARSON CORRELATIONS TMMS-A TMMS-C TMMS-R BSCI-SU BSCI-D BSCI-E BSCI-PL TMMS-A 1 TMMS-C .287** 1 TMMS-R .413** .461** 1 BSCI-SU -.024 -.166** -.188* 1 BSCI-D -.055 -.181** -.198** -.017 1 BSCI-E -.050 -.058 -.199** .054 .222* 1 BSCI-PL -.037 -.193* -.175** -.036 .290** .113* 1 __*p < .05_**p < .001_______________________________________________________________________________________________________________________ Trait Meta-Mood Scale-Attention (TMMS-A), Trait Meta-Mood Scale-Clarity (TMMS-C), Trait Meta-Mood Scale-Repair (TMMS-R), Brief Stress & Coping Substance Use (BSCI-SU), Brief Stress & Coping-Diet (BSCI-D), Brief Stress & Coping-Exercise (BSCI-E), Brief Stress & Coping-Pace of Life (BSCI-PL) • METHODS • PARTICPANTS We looked at the relationships amongperceived emotional intelligence and reported health habits. Participants were college students (N=418) between the ages of 18 and 24, with 41.8% reported freshmen. This analysis was part of a larger study investigating relationships among emotional intelligence, stress, health habits, coping, and eating behaviors in a sample of students at a large Southern Plains university. MEASURES Participants completed web-based questions from the Brief Stress and Coping Inventory (BSCI; Rahe & Tolles, 2002) and the Trait Meta-Mood Scale (TMMS; Salovey, Mayer, Goldman, Turvey, & Palfai, 1995), as well as other measures. For this analysis, we used the Health Habits subscale of the BSCI. In this subscale respondents are asked about health behaviors in four dimensions: (1) Substance Use (“Do you smoke cigarettes”; α = .66), (2) Diet (“Do you eat your meals slowly and calmly”; α = .40), (3) Exercise (“Do you exercise moderately and regularly”; α = .52), and (4) Pace of Life (“Are you in control of the pace of your life”; α = .60). The TMMS measures emotional intelligence as operationalized through the following three constructs: (1) Attention to Feelings (“I pay a lot of attention to how I feel”; α =.84), (2) Clarity of Feelings (“I am usually very clear about my feelings”; α =.81), and (3) Mood Repair (“Although I am sometimes sad, I have a mostly optimistic outlook”; α = .73). STATISTICAL ANALYSES We examined the relationship between participants’ emotional intelligence and reported health habits. We conducted Pearson single-tailed correlations between the three constructs of perceived emotional intelligence (Attention, Clarity, & Repair) and the four areas of health habits (Substance Use, Diet, Exercise, & Pace of Life). Additionally, gender differences were examined on all scales. INTRODUCTION Emotional intelligence is known as the notion that people can recognize their emotional states, remain open to their emotions, monitor and reflect on their emotional states, and mange emotions (Presbury, Echterling, & McKee, 2007). Often hailed to be more important than an intelligence quotient, this construct has produced a wealth of empirical evidence since its foundation. Recently, researchers have suggested that it is important to explore the relationship of the construct of emotional intelligence to other domains than psychological functioning, such as physical health. Theorists differ on how to best assess emotional intelligence. Some researchers use ability-based methods (Brackett, Rivers, Lerner, Salovey, & Shiffman, 2006; Gohm, Corser, & Dalsky, 2005; Lopes, et al., 2004), attempting to capture this construct by using performance based activities. Other researchers elect to use self-report instruments designed to assess perceived traits purportedly central to emotional intelligence (Palmer, Donaldson, & Stough, 2002; Salovey, Stroud, Woolery, & Epel, 2002). Using these different methods, researchers have linked emotional intelligence to coping (Saklofske, Austin, Galloway, & Davidson, 2007), stress (Matthews et al., 2006; Ciarrochi, Deane, & Anderson, 2002), life satisfaction (Palmer, Donaldson, & Stough, 2002; Extremera & Fernandez-Berrocal, 2005), and mood regulation (Gohm, 2003). In the realm of mental health, higher levels of emotional intelligence are associated with lower levels of depression and physical complaints (Salovey, Stroud, Woolery, & Epel, 2002) and lower levels of depression and hopelessness (Ciarrochi, Deane, & Anderson, 2002). In a meta-analysis, Schutte, Malouff, Thorsteinsson, Bhullar, and Rooke (2007) found that “higher emotional intelligence was associated with better health.” They advised more studies need to focus on the relationship between emotional intelligence and physical health. In reviewing the literature on college student health behaviors, we found many areas in which emotional intelligence may play a role. Hudd et al. (2000), found “a relationship between perceived levels of stress among college students, their health habits, health status and self-esteem” (p. 225).Students with high stress and low self-esteem reported less participation in healthy behaviors. Furthermore, the American College Health Association (2006), in a 2005 college student assessment, determined depression and anxiety to be among the top 10 reported health concerns of college students. Stress reportedly was the leading impediment to academic performance among college students (ACHA, 2006). DISCUSSION Although we cannot make a statement of causality, these results indicate a link between the level of perceived emotional intelligence and health-related behaviors. Perception of skill is key to understanding a student’s approach to handling life’s problems. In summary, greater perceived skill at distinguishing between emotions and repairing mood were associated with better health habits. An association of perceived ability to clearly understand emotions and health habits may suggest that those individuals with higher levels of emotional clarity are more aware of their perceived true feelings and thus, are less confused about their mental state. Perceived ability to regulate one’s mood in the face of unpleasant situations perhaps fosters a sense of control over one’s life, allowing for healthier behaviors. Limitations to these results include using a brief measure of health habits and the self-report biases of students. Future research should examine emotional intelligence and a more comprehensive measure of health habits, as well as possible changes over time. With regard to student health, researchers may want to examine sexual behaviors. RESULTS PERCEIVED EMOTIONAL INTELLIGENCE AND HEALTH HABITS Pearson correlation coefficients indicated associations between perceived emotional intelligence and health habits. Specifically, the Clarity of Feelings subscale of the TMMS was negatively correlated with the Health Habits (BSCI) scales of Substance Use (r = -.166, p = .001), Diet (r = -.181, p = .001), and Pace of Life (r =-.193, p = .001). Higher scores on each of the Health Habits scales indicate greater endorsement of unhealthy behaviors. The Mood Repair score was negatively correlated with Substance Use (r =-.188, p = .019), Diet (r =-.198, p = .001), Exercise (r =-.199, p = .001), and Pace of Life (-.175, p = .001). There was no relationship between the Attention to Feelings scale of the TMMS and Health Habits subscales of the BSCI. GENDER CONSIDERATIONS We found gender differences in relation to Attention to Feelings, but not the other TMMS subscales. Independent t-tests showed a significant difference for gender (t = 3.300, p = .001) on Attention to Feelings. As seen in previous research, females showed a higher mean score on Attention to Feelings. IMPLICATIONS Research continues to support the mind-body interaction. Emotional intelligence adds to our understanding of these influences. A report from the American College Health Association (2005) found that “health center medical staff” were the most believable source of health-related information. A multi-disciplinary approach to treating and implementing preventative education may serve as an influential format for universities. Pamphlets and flyers may not be enough. Emotional intelligence, infused with health education, can serve as a powerful tool not only with physical well-being, but also personal growth. Specialized “growth” groups may offer the best chance to provide health education (from trusted educators) and foster emotional awareness. Students can learn from a health professional, interact with their peers, and experience emotional expression/awareness first hand. Problems reported to be of concern for students including depression, anxiety, and stress, should be targeted.