Download
1 / 33
620 likes | 1.78k Views
Acute Kidney Injury. Do we know what we mean?. Definition of AKI. There are more than 35 definitions of AKI (formerly acute renal failure) in literature!

E N D
Acute Kidney Injury Do we know what we mean?
Definition of AKI • There are more than 35 definitions of AKI (formerly acute renal failure) in literature! • Mehta R, Chertow G: Acute renal failure definitions and classification: Time for change? Journal of American Society of Nephrology 2003; 14:2178-2187.
Definition of AKI • RIFLE classification • AKIN classification
RIFLE classification Bellomo R, Ronco C, Kellum J, et al.: Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Initiative (ADQI) Group. Critical Care 2004; 8:R204-R212.
AKIN classification • Modification of the RIFLE classification by Acute Kidney Injury Network (AKIN). • Recognizes that small changes in serum creatinine (>0.3 mg/dl) adversely impact clinical outcome. • Uses serum creatinine, urinary output and time. Coca S, Peixoto A, Garg A, et al.: The prognostic importance of a small acute decrement in kidney function in hospitalized patients: a systematic review and meta-analysis. American Journal of Kidney Diseases 2007; 50:712-720.
AKIN classification *Patients needing RRT are classified stage 3 despite the stage they were before starting RRT Mehta R, Kellum J, Shah S, et al.: Acute kidney Injury Network: Report of an Initiative to improve outcomes in Acute Kidney Injury. Critical Care 2007; 11: R31.
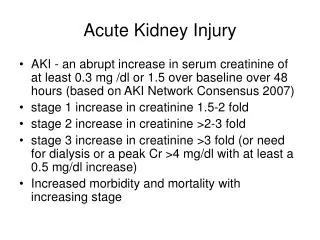
Definition of AKI • AKI is an abrupt (within 48 hrs) reduction in kidney function currently defined as an absolute increase in serum creatinine of ≥ 0.3 mg/dL (≥ 26.4 μmol/L), a percentage increase in serum creatinine of ≥ 50%, or a reduction in urine output (documented oliguria of < 0.5 mL/kg/hr for > 6hrs. Mehta R, Kellum J, Shah S, et al.: Acute kidney Injury Network: Report of an Initiative to improve outcomes in Acute Kidney Injury. Critical Care 2007; 11: R31.
Epidemiology AKI occurs in • ≈ 7% of hospitalized patients. • 36 – 67% of critically ill patients (depending on the definition). • 5-6% of ICU patients with AKI require RRT. Nash K, Hafeez A, Hou S: Hospital-acquired renal insufficiency. American Journal of Kidney Diseases 2002; 39:930-936. Hoste E, Clermont G, Kersten A, et al.: RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: A cohort analysis. Critical Care 2006; 10:R73. Osterman M, Chang R: Acute Kidney Injury in the Intensive Care Unit according to RIFLE. Critical Care Medicine 2007; 35:1837-1843.
Mortality according to RIFLE • Mortality increases proportionately with increasing severity of AKI (using RIFLE). • AKI requiring RRT is an independent risk factor for in-hospital mortality. • Mortality in pts with AKI requiring RRT 50-70%. • Even small changes in serum creatinine are associated with increased mortality. Hoste E, Clermont G, Kersten A, et al.: RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: A cohort analysis. Critical Care 2006; 10:R73. Chertow G, Levy E, Hammermeister K, et al.: Independent association between acute renal failure and mortality following cardiac surgery. American Journal of Medicine 1998; 104:343-348. Uchino S, Kellum J, Bellomo R, et al.: Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005; 294:813-818. Coca S, Peixoto A, Garg A, et al.: The prognostic importance of a small acute decrement in kidney function in hospitalized patients: a systematic review and meta-analysis. American Journal of Kidney Diseases 2007; 50:712-720.
Diagnosis • Serum Creatinine • Urine Output • Time
Limitations of SCr Dennen P, Douglas I, Anderson R,: Acute Kidney Injury in the Intensive Care Unit: An update and primer for the Intensivist. Critical Care Medicine 2010; 38:261-275.
Common causes of AKI in ICU • Sepsis • Major surgery • Low cardiac output • Hypovolemia • Medications (20%) Uchino S, Kellum J, Bellomo R, et al.: Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005; 294:813-818.
Common causes of AKI in ICU • Hepatorenal syndrome • Trauma • Cardiopulmonary bypass • Abdominal compartment syndrome • Rhabdomyolysis • Obstruction Dennen P, Douglas I, Anderson R,: Acute Kidney Injury in the Intensive Care Unit: An update and primer for the Intensivist. Critical Care Medicine 2010; 38:261-275.
Nephrotoxins • NSAIDs • Aminoglycosides • Amphotericin • Penicillins • Acyclovir • Cytotoxics • Radiocontrast dye Dennen P, Douglas I, Anderson R,: Acute Kidney Injury in the Intensive Care Unit: An update and primer for the Intensivist. Critical Care Medicine 2010; 38:261-275.
Prevention of AKI in ICU • Recognition of underlying risk factors • Diabetes • CKD • Age • HTN • Cardiac/liver dysfunction • Maintenance of renal perfusion • Avoidance of hyperglycemia • Avoidance of nephrotoxins Dennen P, Douglas I, Anderson R,: Acute Kidney Injury in the Intensive Care Unit: An update and primer for the Intensivist. Critical Care Medicine 2010; 38:261-275.
Prevention of Contrast-Induced Nephropathy • Avoid use of intravenous contrast in high risk patients if at all possible. • Use pre-procedure volume expansion using isotonic saline (?bicarbonate). • NAC • Avoid concomitant use of nephrotoxic medications if possible. • Use low volume low- or iso-osmolar contrast Dennen P, Douglas I, Anderson R,: Acute Kidney Injury in the Intensive Care Unit: An update and primer for the Intensivist. Critical Care Medicine 2010; 38:261-275.
Prevention of AKI in hepatic dysfunction • Intravenous albumin significantly reduces the incidence of AKI and mortality in patients with cirrhosis and SBP. • Albumin decreases the incidence of AKI after large volume paracentesis. • Albumin and terlipressin decrease mortality in HRS. Sort P, Navasa M, Arroyo V, et al.: Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. New England Journal of Medicine 1999; 341:403-409. Gines P, Tito L, Arroyo V, et al.: Randomised comparative study of therapeutic paracentesis with and without intravenous albumin in cirrhosis. Gastroenterology 1988; 94:1493-1502. Gluud L, Kjaer M, Christensen E: Terlipressin for hepatorenal syndrome. Cochrane Database Systematic Reviews 2006; CD005162.
Management of AKI in ICU • Maintain renal perfusion • Correct metabolic derangements • Provide adequate nutrition • ? Role of diuretics
Maintaining renal perfusion • Human kidney has a compromised ability to autoregulate in AKI. • Maintaining haemodynamic stability and avoiding volume depletion are a priority in AKI. Kelleher S, Robinette J, Conger J: Sympathetic nervous system in the loss of autoregulation in acute renal failure. American Journal of Physiology 1984; 246: F379-386.
Maintaining renal perfusion • Current studies do not include patients with established AKI. • The individual BP target depends on age, co-morbidities (HTN) and the current acute illness. • A generally accepted target remains MAP ≥ 65. Bourgoin A, Leone M, Delmas A, et al.: Increasing mean arterial pressure in patients with septic shock: Effects on oxygen variables and renal function. Critical Care Medicine 2005; 33:780-786.
Volume resuscitation – which fluid? • SAFE study – no statistical difference between volume resuscitation with saline or albumin in survival rates or need for RRT. • Post – hoc analysis – albumin was associated with increased mortality in traumatic brain injury subgroup and improved survival in septic shock patients. Finfer S, Bellomo R, Boyce N, et al.: A comparison of albumin and saline for fluid resuscitation in the intensive care unit. New England Journal of Medicine 2004; 350: 2247-2256.
Volume resuscitation – how much fluid? • Fluid conservative therapy decreased ventilator days and didn’t increase the need for RRT in ARDS patients. • Association between positive fluid balance and increased mortality in AKI patients. Wiedeman H, Wheeler A, Bernard G, et al.: Comparison of two fluid management strategies in acute lung injury. New England Journal of Medicine 2006; 354:2564-2575. Payen D, de Pont A, Sakr Y, et al.; A positive fluid balance is associated with worse outcome in patients with acute renal failure. Critical Care 2008; 12: R74.
Which inotrope/vasopressor? • There is no evidence that from a renal protection standpoint, there is a vasopressor agent of choice to improve kidney outcome. Dennen P, Douglas I, Anderson R,: Acute Kidney Injury in the Intensive Care Unit: An update and primer for the Intensivist. Critical Care Medicine 2010; 38:261-275.
Renal vasodilators? • “Renal” dose dopamine doesn’t reduce the incidence of AKI, the need for RRT or improve outcomes in AKI. • It may worsen renal perfusion in critically ill adults with AKI. • Side effects of dopamine include increased myocardial oxygen demand, increased incidence of atrial fibrillation and negative immuno-modulating effects. Lauschke A, Teichgraber U, Frei U, et al.: “Low-dose” dopamine worsens renal perfusion in patients with acute renal failure. Kidney 2006; 69:1669-1674. Argalious M, Motta P, Khandwala F, et al.: “Renal dose” dopamine is associated with the risk of new onset atrial fibrillation after cardiac surgery. Critical Care Medicine 2005; 33:1327-1332.