Download
1 / 18
180 likes | 314 Views
Deep breath and blow - the HCA role in respiratory care. Hilary Andrews Nurse Advisor Woodlands Health Centre Paddock Wood, Kent. Respiratory Care. Lung Function Tests Peak Flow (PEFR) Asthma Spirometry COPD – Monitoring, QOF Reversibility testing – to exclude asthma

E N D
Deep breath and blow- the HCA role in respiratory care Hilary Andrews Nurse Advisor Woodlands Health Centre Paddock Wood, Kent
Respiratory Care • Lung Function Tests • Peak Flow (PEFR) • Asthma • Spirometry • COPD – Monitoring, QOF • Reversibility testing – to exclude asthma • Opportunistic – Over 35yrs, asthmatic coughing smokers • Health Promotion
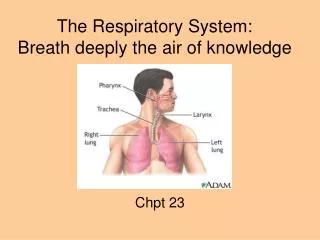
The Respiratory System Nasal Cavity Pharynx Larynx Trachea Right Bronchus Left Bronchus Left Lung Right Lung Heart Position
Asthma • Tightening of muscles surrounding bronchiole causes Bronchospasm • Allergens cause inflammation which further narrows airway • Secretions
COPD • Chronic Obstructive Airways Disease • Umbrella term for Emphysema and Chronic Bronchitis • Walls of alveoli break down with loss of surface area
Pack Years An estimation of the amount someone has smoked Dyspnoea Difficulty Breathing Orthopnoea Breathlessness relieved by sitting upright LTOT Long Term Oxygen Therapy Expectorating Coughing up sputum Haemoptysis Coughing up blood Exacerbation Increase in severity of a disease Cyanosis Blueness of skin Transcutaneous Oxygen Saturation Concentration of oxygen in the blood measured through the skin FEV1 Forced Expiratory Volume in 1 second (often expressed as % predicted) FVC Forced Vital Capacity (often expressed as % predicted) Preventers Medication given to prevent inflammation of airways eg steroids Relievers Medication given to relieve obstructed airways eg bronchodilators – salbutamol CXR Chest X-ray Other respiratory terms
PEFR • Peak Flow demonstrates maximum flow rate of lungs • What device is used? • Peak Flow Meter • Technique? • ‘Fast Blast’ not ‘Slow Blow’ • Limitations • Insufficient effort • Poor seal • Not horizontal • When can it be performed? • Anytime, at home, in surgery, after exercise etc • PEFR Diary
Spirometry • Spirometry demonstrates airflow obstruction • New Diagnosis COPD • Monitoring COPD • Devices • Contraindications • Technique & Accuracy
Contraindications to Spirometry • Pneumothorax or within 2 weeks of resolution • Following recent MI • Unstable angina • Haemoptysis • Following recent eye surgery • Following recent abdominal or thoracic surgery • Following recent CVA • Previous vasovagal episodes • Cervical Disc problems • Ruptured tympanic membrane in last 6 months
Other points to consider prior to Spirometry • Chest infection in last four weeks • Alcohol in last four hours • Vigorous exercise in last 30 minutes • Is clothing restrictive? • Large meal eaten in previous 2 hours?
Technique and Accuracy • Calibration of spirometer • New mouthpiece • Checklist • Prepare the patient • Standing preferably • Breathe in as deeply as possible • Blow breath out forcibly, as hard and fast as possible • Keep blowing! • Repeat at least twice • Check for consistency in trace • Store or print results
Identifying abnormal spirometry traces Slow start to forced expiration Coughing during exhalation Early stoppage of test Extra breath taken during test
Health Promotion • 900,000 people diagnosed with COPD in UK • 450,000 estimated as being undiagnosed • Cost of COPD to NHS • £982,000,000 estimated cost/year (2004)
Health Promotion Therefore:- • Smoking • Offer help to stop smoking at every opportunity • Smoking cessation allows the rate of decline in lung function to return to that of non-smoker • Recognition of other problems that may be affecting the patients quality of life
For more information • ‘Spirometry in practice - A practical guide to using spirometry in primary care’ • The BTS COPD Consortium www.brit-thoracic.org.uk • www.patient.co.uk • www.wipp.nhs.uk