Download
1 / 1
10 likes | 133 Views
No. 064. Renal artery embolisation prior to radical nephrectomy; A retrospective analysis of 42 cases. W. ANDERSON, H. ZARGAR and M. RICE Department of Urology, Auckland City Hospital, New Zealand. Introduction

E N D
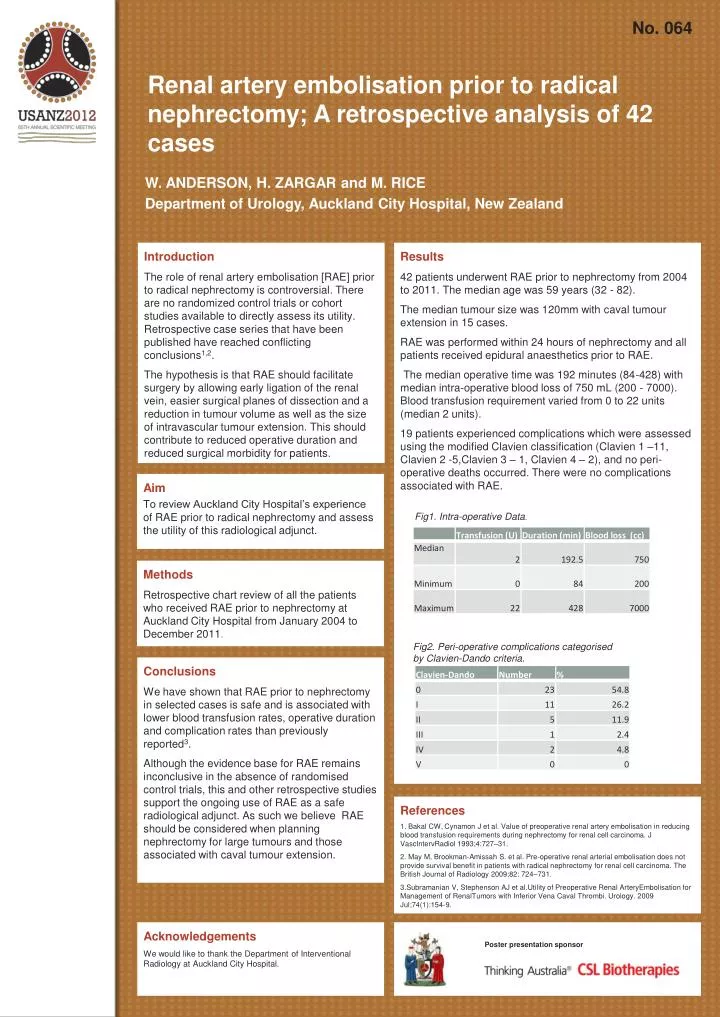
No. 064 Renal artery embolisation prior to radical nephrectomy; A retrospective analysis of 42 cases W. ANDERSON, H. ZARGAR and M. RICE Department of Urology, Auckland City Hospital, New Zealand Introduction The role of renal artery embolisation [RAE] prior to radical nephrectomy is controversial. There are no randomized control trials or cohort studies available to directly assess its utility. Retrospective case series that have been published have reached conflicting conclusions1,2. The hypothesis is that RAE should facilitate surgery by allowing early ligation of the renal vein, easier surgical planes of dissection and a reduction in tumour volume as well as the size of intravascular tumour extension. This should contribute to reduced operative duration and reduced surgical morbidity for patients. Results 42 patients underwent RAE prior to nephrectomy from 2004 to 2011. The median age was 59 years (32 - 82). The median tumour size was 120mm with caval tumour extension in 15 cases. RAE was performed within 24 hours of nephrectomy and all patients received epidural anaesthetics prior to RAE. The median operative time was 192 minutes (84-428) with median intra-operative blood loss of 750 mL (200 - 7000). Blood transfusion requirement varied from 0 to 22 units (median 2 units). 19 patients experienced complications which were assessed using the modified Clavien classification (Clavien 1 –11, Clavien 2 -5,Clavien 3 – 1, Clavien 4 – 2), and no peri-operative deaths occurred. There were no complications associated with RAE. Aim To review Auckland City Hospital’s experience of RAE prior to radical nephrectomy and assess the utility of this radiological adjunct. Fig1. Intra-operative Data. Methods Retrospective chart review of all the patients who received RAE prior to nephrectomy at Auckland City Hospital from January 2004 to December 2011. Fig2. Peri-operative complications categorised by Clavien-Dando criteria. Conclusions We have shown that RAE prior to nephrectomy in selected cases is safe and is associated with lower blood transfusion rates, operative duration and complication rates than previously reported3. Although the evidence base for RAE remains inconclusive in the absence of randomised control trials, this and other retrospective studies support the ongoing use of RAE as a safe radiological adjunct. As such we believe RAE should be considered when planning nephrectomy for large tumours and those associated with caval tumour extension. References 1. Bakal CW, Cynamon J et al. Value of preoperative renal artery embolisation in reducing blood transfusion requirements during nephrectomy for renal cell carcinoma. J VascIntervRadiol 1993;4:727–31. 2. May M, Brookman-Amissah S. et al. Pre-operative renal arterial embolisation does not provide survival benefit in patients with radical nephrectomy for renal cell carcinoma. The British Journal of Radiology 2009;82: 724–731. 3.Subramanian V, Stephenson AJ et al.Utility of Preoperative Renal ArteryEmbolisation for Management of RenalTumors with Inferior Vena Caval Thrombi. Urology. 2009 Jul;74(1):154-9. Acknowledgements We would like to thank the Department of Interventional Radiology at Auckland City Hospital. Poster presentation sponsor