Download
1 / 26
270 likes | 495 Views
Audit of warfarin reversal in over-anticoagulated patients. D Wright and J Seal Department of Haematology Pontefract General Infirmary. Nov 2002. Bleeding during warfarin therapy Risk factors. Age High target INR Actual INR PMH of bleeding CVA Hypertension Alcohol/liver disease.

E N D
Audit of warfarin reversal in over-anticoagulated patients D Wright and J Seal Department of Haematology Pontefract General Infirmary Nov 2002
Bleeding during warfarin therapyRisk factors • Age • High target INR • Actual INR • PMH of bleeding • CVA • Hypertension • Alcohol/liver disease
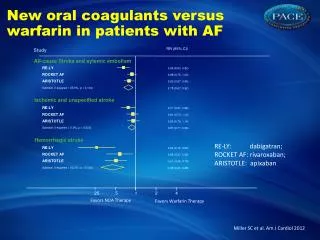
Risk of bleeding whilst on warfarinISCOAT study Prospective study of 2745 patients Bleeding complications: All 7.6 per 100 patient years Major 1.1 per 100 patient years Fatal cerebral bleeds 0.25 per 100 patient years Age > 70 : 10.5 per 100 patient years < 70 : 6 per 100 patient years
Risk of bleeding whilst on oral anticoagulation ISCOAT study: Lancet 1996
Aim of study • Establish a baseline audit of historical practice of warfarin omission in patients with INR>8 • Assess feasibility of using oral vitamin K to reverse anticoagulation in patients with INR>8
Methods • Patients attend community phlebotomy clinics for venous blood sampling. • At this visit patient completes a record sheet detailing warfarin dose, change in medication, clinical condition and any bleeding symptoms. • Samples are sent to central lab for INR testing, along with record sheet. Results are downloaded to A/C computer. BMS reviews results.
INR OVER 8.0 • Significant bleeding symptoms – refer to A/E • No Bleeding – inform Clinical Haematologist • Give 2mg oral dose Vitamin K (KONAKION) • See separate SOP for prescription • Warfarin discontinued temporarily
INR OVER 8.0 • Arrange for INR next day. Repeat INR daily until INR <6.0 • If INR remains over 8.0 repeat Vitamin K • If patient unable to receive Vitamin K discontinue for 3 days and re-check INR • Complete a case report • Send a fax to inform GP
INR 7.1 – 8.0 • Significant bleeding symptoms – refer to A/E • No bleeding proceed as follows • Stop Warfarin for 3 days and re-check INR • Advise patient to attend A/E if bleeding develops
INR 7.1 – 8.0 • Send a fax to inform GP • Recommence warfarin when INR is back in the therapeutic range • Complete a case report
Restarting Warfarin • If over anticoagulation is clearly secondary to a transient event, which has now resolved, then restart Warfarin at the previous maintenance dose • If the reason for over anticoagulation is unknown or due to a continuing risk factor, then restart at a dose between 20% and 25% less than the previous maintenance dose
Results • Between Feb - Dec 2001 forty-one patients had an INR>8 in the absence of significant bleeding • 20 received oral vitamin K • 21 were managed by Warfarin omission
Clinical events • One patient from each group admitted with bleeding complications • One patient in warfarin omission group had a breakthrough PE
Conclusions • After omitting warfarin in patients with an INR>8, 50% still had a raised INR after 3 days • Oral vitamin K at a 2 mg dose achieved at least comparable results within 24 hours • Both patient groups had unstable INR control for at least 1 week after the event • Use of oral vitamin K was not associated with warfarin resistance