Download
1 / 63
640 likes | 663 Views
Explore the physiological mechanisms regulating the immune system through interactions like antigen-induced responses, affinity maturation, and cellular contact with cytokines. Learn about antibody competition, T-cell interactions, and cytokine effects. Discover how cytokines influence immune responses and the classification of cytokines by function. Understand the possibilities of therapeutic interventions affecting the immune system, from stem cell transplantation to gene therapy and immunomodulation.

E N D
Regulation by antigen • Induce immune responses and extinction • Affinity maturation of B lymphocytes • Maintaining immunological memory • Antigenic competition • Threshold density of the complex MHC II-gp Ag on APC
Regulation by antibodies • Antibodiescompeteswiththe BCR for antigen (negative regulatorof B lymphocytestimulating) • IgGimmunecomplexesbind to the BCR andFcgR on B cells, resulting in blockingactivationof B lymphocytes • Regulation via idiotypic network
Regulation by cytokines and cellular contact • InteractionAPC - T lymphocyte • InteractionTH1 – macrophages • InteractionTH2 - B lymphocytes • MutualregulationofactivityTH1 versus TH2 • Developmentof leukocyte subpopulations
Regulation by cytokines and cellular contactInteraction between APC and T cell T cell:TCR - antigen-specific receptor CD4 or CD8 - coreceptor (MHCgp binding) CD 28 - costimulatory receptor (binds CD 80, CD 86) CTLA-4 - inhibitory receptor (binds CD 80, CD 86)
Regulation by cytokines and cellular contactInteraction between TH1 and TH2 cells
Negative regulation of effector cells • CTLA-4 - T cell inhibitory receptor, binds ligands CD80 and CD86 • Self-destruction interaction of the apoptotic receptor Fas with ligand FasL on the surface of activated T lymphocytes • Inhibitory receptors of NK cells
Suppression mediated by T lymphocytes • Mutual negative interactionTH1 and TH2cytokine-mediated • Clonaleliminationoranergyof T lymphocytesaftercontactwith antigen on thesurfaceofothercellsthan APC • Regulatory T cells(Treg, Tr1, Th3 - CD 4+) help to maintain tolerance to autoantigens; produceTGFb, IL-10
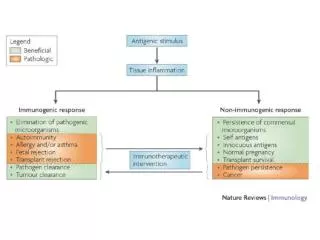
Factors influencing the outcome of the immune response Thesame antigen caninduceanactiveimmune response oranactivestateof tolerance, theresultof response depends on many factors: • Stateoftheimmunesystem • Propertiesof antigen • Doseof antigen • Routeof antigen administration
Cytokines • Regulatory proteins and glycoproteins produced by leukocytes and other cells • Essential regulators of the immune system • Apply also outside the immune system (angiogenesis, tissue regeneration, carcinogenesis, treatment of many brain functions, embryonic development ...) • Cytokines - secreted - membrane (CD 80, CD86, CD40L, FasL ..)
Cytokines • Pleiotropic effect • Operates in a cascade • Cytokine network • Cytokine system is redundant • Effects of cytokines - autocrine - paracrine - endocrine • Are known as interleukins (IL-1…IL-38)(except: TNF, lymphotoxin, TGF, interferons, CSF and growth factors)
B cells communicate via cytokines with other cells, such as T cells and macrophages
Overview of the most important cytokines MF – macrophages; M – monocytes; N – neutrophils; DC – dendritic cells; NK – natural killers; L – lymphocytes; B – B cell; T – T cell
Clasification of cytokines by functions • Proinflammatory cytokines (IL-1, IL-6,IL- 8,IL- 12,IL- 18, TNF) • Antiinflammatory cytokines (IL-4, IL-10, TGF) • Cytokines with the activity of hematopoietic cells growth factor (IL-2, 3, 4, 5, 6, 7, 9, 11, 14, 15, CSF, SCF, LIF, EPO) • Cytokines applying in TH2 humoral immunity (IL-4, 5, 9, 13) • Cytokines applying in the cell-mediated immunity TH1 (IL-2, 12, IFN, GM-CSF, lymphotoxin) • Cytokines with anti-viral effect (IFN-, IFN-, IFN- )
Cytokine receptors • Consistingof 2 or 3 subunits • Onesubunitbindscytokine, other are associatedwithcytoplasmicsignalingmolecules (protein kinases) • Signalingsubunitisshared by severaldifferentcytokinereceptors - called receptor family • Signalingthrough these receptorsmaylead to proliferation, differentiation, activationofeffectormechanismsorblockingthe cell cycleandinductionofapoptosis
Causal treatment a) Stem cell transplantation • treatmentof severe congenitaldisordersoftheimmunesystemandsomelymphoproliferativeandmyeloproliferativedisorders • complications: infectiouscomplicationsGraft-versus-host disease • obtaining stem cells - from bone marrow - fromumbilicalcordblood - fromperipheralblood
Causal treatment b) Gene therapy • transductionof the missing gene to hematopoietic stem cells using viralvectors • used as a treatmentfor 2 formsof SCID
Substitution treatment • autologous stem cell transplantation (following chemotherapy and radiotherapy) • treatment with intravenous immunoglobulin (derived from plasma of blood donors) • substitution of C1 inhibitor for hereditary angioedema • substitution of erythropoietin in patients with chronic renal failure • substitution of G-CSF in agranulocytosis
Immunomodulation = medicalprocedure to adjustthedisruptedimmunefunction Non-specificimmunosuppression • nonspecific = affects not onlyautoreactiveandaloreactivelymphocytes, butalsoothercomponentsofimmunity (risk ofreductionantiinfectiousandantitumorimmunity) • usedfortreatmentofautoimmunediseases, for organ transplantationand severe allergicconditions
Non-specific immunosuppression Corticosteroids • anti-inflammatory, immunosuppressive effects • suppress the expression of some genes (IL-2, IL-1, phospholipase A, MHC gp II, adhesion molecules) • inhibition of histamine release from basophils • higher concentrations induce apoptosis of lymfocytes
Non-specific immunosuppression Immunosuppressants affecting the metabolism of DNA (cytostatics) • cyclophosphamide (alkylating agent) • methotrexate (antimetabolite) • azathioprine (purine analogue)
Non-specificimmunosuppression Immunosuppressantselectivelyinhibiting T cells • immunosuppressive ATB: cyclosporine A, tacrolimus, rapamycin(suppressingtheexpressionof IL-2 and IL-2R in activated T lymphocytes) • anti-CD3 monoclonalantibody(imunosuppressionaftertransplantation, treatmentofrejectioncrises)
Non-specificimmunosuppression Immunoglobulins in the immunosuppressive indication • polyspecific intravenous immunoglobulins • inhibition of B lymphocytes • antiidiotype activity • inhibition of cytokines • neutralization of toxins • inhibition of complement activation
Anti-inflammatory and antiallergic treatment • nonsteroidal anti-inflammatory drugs • antihistamines- blocking H1 receptor - reduce the expression of adhesion molekules - reduce the secretion of histamine ... • inhibitors of inflammatory cytokine- monoclonal antibodies against TNF - thalidomide (TNF inhibitor) • Anti IgE antibodies (omalizumab) - severe allergic astma
Non-specific immunostimulant therapy • synthetic immunomodulators • Methisoprinol (Isoprinosine) - used in viral infections with more severe or relapsing course • bacterial extracts and lysates • Broncho-Vaxom - prevention of recurrent respiratory tract infections • Ribomunyl • products of the immune system • IL-2 - renal adenocarcinoma • IFNa, IFNb - viral hepatitis, some leukemia • Erythropoietin – renal failure • G-CSF, GM-CSF – neutropenia • Transfer factor (blood donors leukocytes undergoing dialysis) • Thymus hormones
Antigen-specific immunomodulation • specificimmunomodulation = induceofanimmune response or tolerance to a specific antigen • activeimmunization • passiveimmunization • specificimmunosuppression
Antigen-specific immunomodulation Activeimmunization (vaccination)= the induction of immunity after exposure toan antigen • activatesspecificcellularandhumoralimmunity • createslong-term immunity (memorycells) • protectagainst a pathogenbearingthis antigen orsimilar antigen (prophylaxis)
Antigen-specific immunomodulation active immunization (vaccination) • vaccines are made from inactivated or attenuated microorganisms or their antigens (polysaccharide capsule, toxins) • attenuated vaccines cannot be used by immunocompromised individuals • risk of infection or anaphylactic reactions
Antigen-specific immunomodulation Passiveimmunization • natural- transfer ofmaternalantibodies in fetalblood • therapeutically - the use ofanimalantibodiesagainstvarioustoxins(snaketoxins, tetanus toxin, botulinum toxin) • prophylaxis - thehumanimmunoglobulinfromimmunizedindividuals (hepatitis A, rabies, tetanus) - Anti-RhDantibodies – preventimmunizationofmotherwithRhD+ fetus erythrocytes • provides a temporary (3 weeks) specifichumoralimmunity • the risk anaphylacticreactions
Antigen-specific immunomodulation Specific immunosuppression= induction of tolerance to a specific antigen • induction of tolerance by oral administration of antigen (treatment of certain autoimmune diseases) • allergen immunotherapy (pollen, insect poisons) Vaccination against cancer • immunization by dendritic cells
Defence against extracellular pathogens • bacteria (gram-negative, gram-positive cocci, bacilli), unicellularparasites • pathogensinduceinflammation • removed by phagocytosis - neutrophilgranulocytes • opsonization (IgGandIgAantibodies, C3b, lectins, CRP...)
Defence against extracellular pathogensOpsonisation and phagocytosis
Defence against extracellular pathogens • Phagocytes are attracted to thesiteofinfection by chemotacticsubstances(C5a, C3a andchemotacticproductsofbacteria…) • ingestedbacteria are destroyed by themicrobicidalsystems(productsof NADP-H oxidase, hydrolyticenzymesandbactericidalsubstances in lysosomes) • phagocytesproduceproinflammatorycytokines(IL-1, IL-6, TNF)
Defence against extracellular pathogens • IgM - complement activation • IgG - complement activation, opsonization • IgA - opsonizationsIgA prevents against infection by intestinal and respiratory bacteria • in the defense against bacterial toxins apply neutralizing antibodies (Clostridium tetani and botulinum …)
Defence against extracellular pathogens • "indirect toxins - bacterial Lipopolysaccharide (LPS) stimulates big number of monocytes to release TNF, which can cause septic shock • individuals with immunodeficiency of phagocytes, complement and antibodies production are especially at risk of infections with extracellular bacterial
Defense against intracellular pathogens • bacteria, fungi and unicellular parasites • intracellular parasites are resistant to the microbicidal mechanisms of phagocytes • macrophages, which absorbed them, produce IL-12 → TH1 differentiation, production of IFNg and membrane TNF → activation of macrophages and production of NO
Defense against intracellular pathogens • TClymphocytesapply in the defense againstintracelularparasites, whichescapefromphagolysosomes • individualswithcertaindisordersofphagocytesanddefectsof T lymphocytes are at risk ofinfectionswithintracellularmicroorganisms
Anti-viral defence • interferons - productionofIFNaandIFNbisinduced in infectedcells; IFNgactivatesmacrophages (iNOS) • IFNaandIFNb -preventsviralreplication - induceproliferationofNK cells - increase the expression of HLA-I
Anti-viral defence • NK cells - ADCC (Antibody-dependent cell-mediated cytotoxicity); NK cell bind with CD16 (Fcg receptor) to IgG which has bound to the surface of infected cell and then NK cell release perforins and granzymes (degranulation) • infected macrophages produce IL-12 (a strong activator of NK cells)
Anti-viral defence • in the defense againstcytopathicvirusesappliedantibodies: • sIgAinhibitmucosaladhesionofviruses (defense againstrespiratoryvirusesandenteroviruses) • neutralizingIgGandIgMantibodiesactivatetheclassicalpathwayofcomplement, thatisable to lyse certainviruses • opsonizedviralparticles are phagocytosed • IgAandIgGhavepreventiveeffect in secondaryviralinfection