Download
1 / 40
440 likes | 1.07k Views
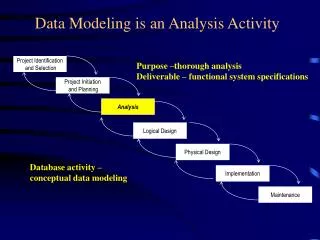
Lab Activity 19 & 20. Cranial Nerves General Senses. Portland Community College BI 232. Cranial Nerves. Nerves that originate from the brain rather than the spinal cord Part of the peripheral nervous system (not the central nervous system) May contain one or more of the following: Sensory

E N D
Lab Activity 19 & 20 Cranial Nerves General Senses Portland Community College BI 232
Cranial Nerves • Nerves that originate from the brain rather than the spinal cord • Part of the peripheral nervous system (not the central nervous system) • May contain one or more of the following: • Sensory • Somatic Motor (voluntary movement) • Parasympathetic Motor (involuntary “rest and digest” part of the autonomic nervous system)
CN I: Olfactory Nerve • Function: • Sensory for smell • Test: Have patient identify aromatic substances like vanilla or coffee (avoid irritating substances like smelling-salts, cloves, mint) • Symptoms of nerve damage: Anosmia: diminished or absent sense of smell
CN II: Optic Nerve • Function: • Sensory for vision • Tests: • Eye chart • Check peripheral vision • Funduscopic exam
CN II: Optic Nerve • Optic chiasm: Fibers from the nasal half of each retina cross over to the opposite side of the brain. • Symptoms of nerve damage: • Loss of vision (peripheral or central) • Abnormal funduscopic appearance
CN II: Optic Nerve Pathology Papilledema. Note swelling of the disc, hemorrhages, and exudates, with preservation of the physiologic cup. Proliferative Diabetic Retinopathy. Note the multiple hemorrhages throughout the retina.
Originates in the midbrain CN III: Oculomotor nerve • Function: • Somatic Motor to extraocular muscles (voluntarily move the eye) • Parasympathetic (motor) to iris and lens (pupillary constriction) • Tests: • Check pupils for size, shape and equality • Shine light in each eye and check for pupil constriction • Have patient follow an object in all directions to check for symmetric eye movements
CN III: Oculomotor Nerve Injury • Symptoms of nerve damage: • Double vision (diplopia): The affected eye turns outward when the unaffected eye looks straight ahead • The affected eye can move only to the middle when looking inward and cannot look upward and downward. • Ptosis: eyelid droop • Pupil may be dilated and sometimes fixed
Oculomotor Nerve Injury Right Eye Injured side Normal side
Pupillary Reflex Efferent Afferent Consensual reflex: Both pupils should constrict at the same time
Originates in the midbrain CN IV: Trochlear Nerve • Function: • Somatic motor to superior oblique muscle of the eye. • Test: Check eye movements • Symptoms of nerve damage: • Outward rotation of the affected eye • Vertical diplopia Normal side Injured side
Originates in the pons CN VI: Abducens Nerve • Function: • Somatic Motor to lateral rectus muscle of the eye. • Test: Check eye movements • Symptoms of nerve damage: • The affected eye will tend to be deviated inward because of the unopposed action of the medial rectus muscle. • Cannot move eyeball laterally beyond the midpoint Normal side Injured side
CN V: Trigeminal Nerve 3 Branches • Ophthalmic • Maxillary • Mandibular
Originates in the pons CN V: Trigeminal Nerve • Function: • Somatic Motor (mandibular branch) to muscles of mastication (chewing) • Sensory (all branches)to face and cornea.
CN V: Trigeminal Nerve Test: Have patient bite down while you palpate the masseter muscle Test: Touch patient with an open paperclip and ask “sharp or dull” Test: Touch cornea with a wisp of cotton. Patient should blink
CN V: Trigeminal Nerve • Symptoms of nerve damage: • Inability to firmly bite down (mandibular branch only) • Loss of sensation (each branch can be affected independently) • Loss of corneal reflex (may indicate brain stem injury) • Trigeminal Neuralgia (Tic Douloureux): debilitating intermittent pain on one side of the face
Originates in the pons CN VII: Facial Nerve 5 Branches • Temporal • Zygomatic • Buccal • Mandibular • Cervical • Function: • Somatic Motor to muscles of facial expression • Parasympathetic (motor) to lacrimal and salivary glands • Sensory taste to anterior 2/3 tongue
CN VII: Facial Nerve Testing • Tests: • Check taste on anterior 2/3 of tongue by having patient taste sugar, salt, sour and bitter • Check symmetry of facial muscles: • Close eyes, smile, whistle, puff out cheeks (make funny faces) • Check tearing with ammonia fumes
CN VII: Facial Nerve • Symptoms of nerve damage: • Mild weakness to total paralysis of facial muscles (may include twitching), • Drooping eyelid • Drooping corner of the mouth • Drooling or dry mouth • Impairment of taste • Excessive tearing in the eye or dry eye
CN VII: Facial Nerve Injury (Bell’s Palsy) Paralyzed facial muscles Normal side Injured side Patients can still feel their face because sensory is supplied by the trigeminal nerve
Originates in the medulla CN VIII: Vestibulocochlear • Function:Sensory • Vestibular system for balance & equilibrium • Cochlea for hearing • Tests: • Auditory component of the nerve: • Hearing test • Vestibular control of balance and movement: • Romberg test (tests equilibrium)
CN VIII: Vestibulocochlear Tests • Simple hearing test: • Rub fingers together near the ear and ask “right or left” If there is lateralization (hearing louder on one side) there is a problem • Other hearing tests: • Performed by an audiologist with special equipment to determine tones, frequencies and degree of hearing loss
CN VIII: Vestibulocochlear TestsRomberg Test • Have patient stand with arms at side and feet together • Have patient stand with their eyes closed • Stand close to prevent falls • Normally, they should maintain position for 20 seconds with only minimal swaying • If they loose their balance, they have failed the equilibrium test.
CN IX: Glossopharyngeal • Function: • Somatic Motor to muscles of pharynx • Parasympathetic (motor) to salivary glands • Sensory to pharynx and taste to posterior tongue
Originates in the medulla CN IX: Glossopharyngeal • Tests: • Gag reflex: Touch each side of the throat with the tongue depressor • Evaluate swallowing movements • Say AHH, and watch the palate and uvula elevate. • Evaluate taste on posterior 1/3 of tongue • Symptoms of nerve damage: • Loss of gag reflex • Difficulty swallowing • Loss of taste
Originates in the medulla CN X: Vagus Nerve • Function: • Somatic Motor to muscles of pharynxand larynx • Parasympathetic (motor) fibers of the heart and other viscera • Sensory to pharynx and larynx
CN X: Vagus Nerve • Test: • Inspect palate • Test gag reflex • Symptoms of nerve damage: • Loss of gag reflex • Difficulty swallowing • Hoarse voice
Originates in the medulla CN XI: Accessory Nerve • Function:Somatic Motor to sternocleidomastoid and trapezius muscles
CN XI: Accessory Nerve • Test: • Shrug shoulders against resistance • Turn head against resistance.
CN XI: Accessory Nerve • Symptoms of nerve damage: • Weakness • Uneven shoulders • Winged scapula
Originates in the medulla CN XII: Hypoglossal Nerve • Function:Somatic Motor to tongue
Hypoglossal Nerve Injury • Test: • Ask patient to stick out tongue • Symptoms of nerve damage: • When paralyzed, the tongue will point to the damaged side Normal side Injured side
Lab Activity 20 General Senses
General Senses: Receptors • Nociceptors: Pain receptors • Thermoreceptors: Temperature receptors (free nerve endings) • Chemoreceptors: Detect small changes in the concentration of specific chemicals or compounds • Mechanoreceptors: Sensitive to stimuli that distort their cell membranes (contain mechanically gated ion channels) • Tactile receptors • Baroreceptors • Proprioceptors
Classes of Mechanoreceptors • Tactile receptors: sensations of touch, pressure and vibration • Free nerve endings • Root hair plexus • Tactile discs (Merkel’s discs) • Tactile corpuscles (Meissner’s corpuscles) • Lamellated corpuscles (Pancinian corpuscles) • Baroreceptors: Detect pressure changes in the walls of blood vessels and portions of the digestive, reproductive and urinary tracts • Proprioceptors: Monitor the positions of joints and muscles.
Pancinian Corpuscle (aka: Lamellated Corpuscle) • Lie deep in the dermis • Respond only when deep pressure is first applied • Monitor high frequency vibrations
Meissner’s Corpuscle (aka: Tactile Corpuscle) • Lie in the dermal papillae of the skin • Respond to light touch
The End The End