Download
1 / 43
460 likes | 573 Views
This article by Dr. Christian Veillette covers the epidemiology, pathoanatomy, diagnosis, and management options of anterior glenohumeral instability, with special emphasis on surgical procedures and prognostic variables. Learn about mechanisms of injury, classification, and natural history in detail.

E N D
Anterior Glenohumeral Instability Christian Veillette M.D., M.Sc., FRCSC Assistant Professor, University of Toronto Shoulder & Elbow Reconstructive Surgery Toronto Western Hospital University Health Network Email: orthonet@gmail.com
Objectives • Epidemiology • Natural History • Pathoanatomy • Diagnosis • History, Physical Exam, Imaging • Management Options • Consideration, Indications, Complications • Surgical Procedures • Cases
Introduction • Incidence – 2% over lifetime - Hovelius (CORR 1982); Simonet (CORR 1984) • Anterior dislocations account for ~95% of shoulder dislocations • Typically occurs in athletes who are < 25 years old • Males are much more commonly affected than are females (85-90%) • Pathology most commonly found in shoulders following a dislocation is a Bankart lesion • Disruption of the labrum and the contiguous anterior band of the inferior glenohumeral ligamentous complex (IGHLC) • Bankhart lesion occurs > 85% of the time
Mechanism of Injury • Most common mechanism of injury is a fall onto an outstretched arm • Extremity is typically in an externally rotated and abducted position • Places the anterior structures at greatest risk for failure (especially the inferior glenohumeral ligament) • Other mechanisms: • elevation combined with external rotation • direct blow
Classification • Instability can be classified by: • direction of instability (anterior, posterior, multidirectional) • degree of instability (subluxation, dislocation) • etiology (traumatic, atraumatic, overuse) • timing (acute, recurrent, fixed) • TUBS and AMBRI (Matsen) • TUBS or “Torn Loose” • Traumatic aetiology, Unidirectional instability, Bankart lesion is the pathology, Surgery is required • AMBRI or “Born Loose” • Atraumatic: minor trauma, Multidirectional instability may be present, Bilateral: asymptomatic shoulder is also loose, Rehabilitation is the treatment of choice, Inferior capsular shift: surgery required if conservative measures fail
Prognostic variables • Gender – No correlation if look at <30 yrs of age group • Hand dominance - No correlation consistently reported • Initial Trauma - Controversial whether amount of initial trauma correlates with recurrence • Sports participation - Likely that level and type of sport participation correlates with recurrence rate • Initial X-ray Appearance – GT # low rate • Period of immobilsation – Unclear whether period of immobilization corrrelates with recurrence rate • Age – Strong correlation between age and recurrence in all studies
Age & Recurrence Rate • McLaughlin and Cavallaro (Am J Surg 1950) • 573 patients - 90% in patients < 20 y, 60% in patients 20-40 y, only 10% in patients > 40 y • Rowe (Orthop Clin North Am 1980) • 94% in patients < 20 y, 74% in patients 20-40 y • Henry and Genung (Am J Sports Med 1982) • 121 patients - 88% regardless of type of nonoperative treatment • Simonet and Cofield (Am J Sports Med 1984) • 116 patients - 66% in patients < 20 y, 40% in patients 20-40 y • Arciero et al (Am J Sports Med 1984) • 80% in 15 student-athletes with average age of 20 y
Natural History • Bilaterality - <30 y at time of first dislocation • 18% bilaterality within 10 yrs (Hovelius, JBJS 1996) • Osteoarthritis - Risk of OA regardless of recurrence or surgery at 10 y • mod. to severe 9% (Hovelius, JBJS 1996) • mild 11% • 17% (Lill, Chirurg 1998) • Functional Disability (Tsai et al, Am J Sports Med 1991) • ~ 60% of patients with anterior instability complained of poor strength, decrease range of motion, increased pain after conservative treatment
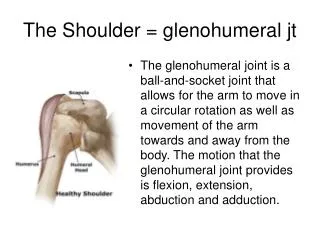
Anatomy • humeral head is retroverted 30o • typical neck-shaft angle is 130o • glenoid fossa average radius of curvature is 24 mm, only 2 mm less than humeral head • less than one-third of the humeral head articulates with glenoid during any given position of rotation • glenohumeral articulation is minimally constrained by bony anatomy alone • glenoid labrum is a fibrocartilaginous structure • functionally deepens the glenoid fossa • serves as an anatomic restraint to humeral head translation • provides an anchor point for the glenohumeral ligaments • stability is conferred by a series of dynamic and static soft tissue restraints
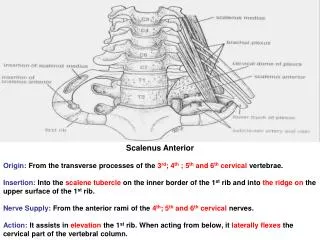
Shoulder Stabilisers - Static • Intracapsular pressure • Suction effect: glenoid labrum acting on humeral head like a “plunger” • Adhesion-cohesion: between 2 wet smooth surfaces • Glenoid version • Humeral retroversion: normal 21-30º, some studies have shown a significant reduction in patients with recurrent anterior dislocation • Labrum: “chock block” to humeral head movement, increases depth of the glenoid by 50% • Ligaments – main static restraints • Coracohumeral ligament • Superior glenohumeral ligament (SGHL) • Middle glenohumeral ligament (MGHL) • Inferior glenohumeral ligament complex (IGHLC) – “hammock” • Posterosuperior capsule Primary static stabilizer limiting anterior movement of the shoulder in 90 degrees of abduction is the IGHL complex
Shoulder Stabilisers - Dynamic • Rotator cuff • Subscapularis muscle provides stability at lower degrees of abduction but contributes little when shoulder is in 90o abduction • Rotator cuff compresses humeral head into glenolabral socket, contributing stability, esp. in middle ROM when ligaments are lax • Proprioception • Lephart et al 1994 studied proprioception in three groups of patients: Normal, Unstable, Reconstructed shoulders • Proprioception was significantly reduced in unstable shoulders but returned to near normal in reconstructed shoulders • Long head of biceps: biceps is much more active in patients with recurrent dislocation
Pathophysiology • pathologic lesions leading to the unstable shoulder can be divided into two main groups: • anterior labrum • glenohumeral capsule
Anterior Labrum • Bankart lesion • classically described as the detachment of the anteroinferior labrum with its attached inferior glenohumeral ligament complex • Initially felt that this detachment was the “essential lesion” • Speer et al. • Created Bankhart lesion from 12 o’clock to 6 o’clock and found minimal translation (<4 mm) • Capsular injury also required to dislocate shoulder
Glenohumeral Capsule • Turkel 1981 • Selective cutting study showed importance of GH ligaments • Bigliani et al. 1992 • Cadaveric bone-ligament-bone specimens of the IGHL were created and tested to failure • found that ligament failed • off the glenoid in 40% of the specimens (Bankart) • intrasubstance in 35% • off the humeral side in 25% • Most importantly showed that the capsule underwent plastic deformation prior to failure in all specimens
Patient History • Mechanism of injury is critical in management of dislocated shoulder • Arm position at time of injury helpful in subtle forms of subluxation • if the patient complains of symptoms in the cocking position, anterior subluxation • if the symptoms occur in the follow-through phase, posterior subluxation • Identify the amount of force required • Number of dislocations suffered by the patient • Age at the time of first dislocation is extremely important • most important prognostic indicator for patients with recurrent dislocations.
Exam - Acute Instability • Patients present with severe pain with arm held at side • Normal contour of deltoid and acromion are usually lost • Visual inspection, palpation, strength testing and a thorough neurovascular examination • Specific neurologic testing should include pre-reduction evaluation of axillary, musculocutaneous, median, ulnar, and radial nerves. • Sensation over axillary nerve distribution (lateral aspect of the shoulder) has proven to be quite unreliable. • Isometric contraction of 3 deltoid heads (anterior, middle, and posterior), usually indicates an intact axillary nerve.
Exam - Recurrent Instability • Apprehension test • Anterior release • Anteroposterior translation • Grade 1+ translation to the glenoid rim • Grade 2+ the head subluxes beyond the rim but self-reduces when the force is released • Grade 3+ the head dislocates and does not spontaneously reduce • Sulcus • Ligamentous laxity
Imaging Acute Setting • a true anteroposterior (AP) view, trans-scapular Y view, and axillary view should be obtained to determine the direction of the dislocation • Radiographs should be performed before reduction is attempted unless • the direction of dislocation is known from prior dislocations • the reduction is performed by an experienced physician, trainer, or other health care worker. • Post-reduction radiographs should confirm that the reduction was successful and that there are no acute fractures
Imaging Recurrent Instability • Several special views may be more helpful with recurrent instability • AP radiograph in internal rotation, Stryker-notch views are used to visualize Hill-Sachs lesion • West Point axillary view used to visualize anteroinferior glenoid (Bankart), avoids superimposition of the coracoid process & clavicle
Intra-articular lidocaine vs. IV sedation for closed reduction? Miller et. al. J Bone Joint Surg Am. 2002 Dec;84-A(12):2135-9. • prospective, randomized study, skeletally mature patients, isolated glenohumeral joint dislocation • IV sedation or intra-articular lidocaine, modified Stimson method • 30 patients • lidocaine group (n=15) - significantly less time in ER (av. time, 75 min vs 185 min in the sedation group, p < 0.01) • no significant difference between groups with regard to pain (p = 0.37), success of Stimson technique (p = 1.00), or time required to reduce shoulder (p = 0.42) • cost of IV sedation was $97.64/patient vs $0.52 for intra-articular lidocaine • Use of intra-articular lidocaine to facilitate reduction with the Stimson technique • safe and effective method • less money, time, and nursing resources
Orlinsky et. al. J Emerg Med. 2002 Apr;22(3):241-5. • compare the analgesic effectiveness of intra-articular lidocaine versus intravenous meperidine and diazepam • Prospective randomized trial • 54 patients with anterior shoulder dislocations • 29 intra-articular lidocaine (IAL) • 25 intravenous meperidine/diazepam (IVMD) • IAL less effective than IVMD in relieving pre-reduction pain (p = 0.045) • IAL equally effective in overall pain relief (p = 0.98) • IAL was more effective than IVMD in shortening recovery time (p = 0.025) • IVMD trend towards physician-perceived muscle relaxation and patient's perception of analgesia adequacy
Kosnik et. Al. Am J Emerg Med. 1999 Oct;17(6):566-70. • prospective, randomized, nonblinded clinical trial • local intraarticular lidocaine injection (IAL) vs intravenous analgesia/sedation (IVAS) • Level 1, trauma center • 49 patients: 20 - IVAS group, 29 - IAL group • No difference between pain scores (IVAS 3.32+/-2.39 vs IAL 4.90+/-2.34, P = .18) • No difference between ease of reduction scores (IVAS 3.32+/-2.36 vs IAL 4.45+/-2.46, P = .12) • IVAS tended to have higher success rate (20 of 20) than IAL (25 of 29) (P = .16). • Reduction rate as a function of time delay in treatment • patients presenting 5.5 h after dislocation more likely to fail treatment with IAL (P = .00001) • Half of the patients in the IAL group who had experience with IVAS did not favor IAL
Is Sling Appropriate? • Non-operative management = Sling immobilzation with the arm internally rotated No evidence • Itoi et al. J Bone Joint Surg Am 2001; 83-A(5): 661-667 • magnetic resonance imaging in patients • Hatrick C, O'Leary S, Miller B, et al. ORS 2002. • load sensors in cadavers
Itoi et. al. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):413-5. • Prospective, nonrandomized trial • 40 patients initial shoulder dislocations • Immobilization in internal rotation (IR group, n = 20) • Immobilization in external rotation (ER group, n = 20) • Recurrence rate @ 15.5 months • 30% in the IR group • 0% in the ER group • Difference in recurrence rate was even greater < 30 years • 45% in the IR group • 0% in the ER group
Role of Early Arthroscopic Repair? Bottoni et. al. Am J Sports Med. 2002 Jul-Aug;30(4):576-80. • Prospective, randomized clinical trial. Army Medical center. • Compared nonoperative treatment with arthroscopic Bankart repair for acute, traumatic shoulder dislocations in young athletes • 14 nonoperatively treated patients - 4 weeks of immobilization + supervised rehab. program • 10 operatively treated patients - arthroscopic Bankart repair (bioabsorbable tack) + same rehab protocol as nonop. patients • Av. follow-up = 36 months, 3 patients lost to follow-up • 9/12 nonoperatively treated patients (75%) developed recurrent instability • 6/9 required subsequent open Bankart repair for recurrent instability • 1/9 operatively treated patients (11.1%) developed recurrent instability
Kirkley A, Griffin S, Richards C, Miniaci A, Mohtadi N. Arthroscopy. 1999 Jul-Aug;15(5):507-14. • Compare effectiveness of traditional treatment vs. immediate arthroscopic stabilization in young patients with first traumatic anterior dislocation of the shoulder • Prospective, randomized, blinded trial • 40 skeletally mature patients < 30 yr • 20 pts, Immobilization for 3 wks + rehabilitation (group T) • 20 pts, Arthroscopic stabilization (< 4 weeks of injury) + immobilization/rehabilitation (group S) • 2 yr follow-up • Rate of redislocation: T = 47%, S = 15.9%, P = .03 • Western Ontario Shoulder Instability (WOSI) index showed significantly better results in the surgically treated group at the 33 months • T = 633.93 v S = 287.1, P = .03 • No significant difference in range of motion
Role of Arthroscopic Lavage? Wintzell et. Al. J Shoulder Elbow Surg. 1999 Sep-Oct;8(5):399-402. • Prospective randomized study, Sweden • Compared treatment results of arthroscopic lavage with results of conventional nonoperative treatment • 30 consecutive patients, traumatic primary anterior shoulder dislocation, 18-30 y, no history of shoulder problems • 2-year follow-up • 3 (20%) of 15 patients in the lavage group had a redislocated shoulder • 9 (60%) of 15 patients in the non-operative group (P = .03) • 2 in lavage group vs. 6 in control group had been operated on or were scheduled for stabilizing surgery • Functional outcome/Constant and Rowe shoulder scores did not reveal any significant difference (P = .07) • Joint effusion decreased more rapidly (33%) in arthroscopic lavage group vs. non-operated group
Indications for Surgery • 1) initial dislocation in a patient who participates in high-risk or high-demand activities in whom recurrent dislocation would be inopportune or dangerous • professional athletes, mountain climbers, certain types of construction workers • 2) recurrence of dislocation or subluxation after trauma treated adequately with nonoperative measures • 3) pain due to recurrent transient shoulder subluxation when the arm is used for overhead activities Gill & Zarins. Am J Sports Med, Jan-Feb, 2003.
Algorithm for Anterior Shoulder Instability J Am Acad Orthop Surg 1997;5:233-239
Nonanatomic Repairs • Bristow • Transfer coracoid process to anteroinferior glenoid • Sling effect and bone block • Putti-Platt • “Pants-over-vest” repair capsule • Magnusen-Stack • subscapularis tendon is detached from its insertion on the lesser tuberosity, transferred laterally to the greater tuberosity • Infrequent indications for using these procedures except in revision surgery
Anatomic Repairs • Restoring normal anatomy is guiding principle in surgery to correct anterior shoulder instability • If the labrum has been detached, it is reattached to the anterior glenoid rim • If the capsule has been stripped off the glenoid neck, the capsule is reattached to the bony glenoid rim • If greater than one-third of the glenoid fossa is involved, a bone block procedure such as a Bristow or iliac crest bone graft may be considered • Guidelines • Anatomic dissection at time of surgery • Identification and repair of lesions responsible for instability • Returning tissues to their anatomic locations • Early postoperative range of motion
Surgical Issues • Incision subscapularis tendon/capsule • Bankart repair • Capsular shift
Complications • Recurrent instability (10%) - most common causes • continued presence of avulsed anterior capsule and labrum from glenoid rim (unrepaired Bankart lesion) • excessive capsular laxity • an enlarged "rotator interval” • failure to diagnose correct direction(s) of instability • Other causes include • presence of a Hill-Sachs lesion • reduced humeral head retroversion • excessive glenoid cavity retroversion • avulsion of the anterior capsule from its lateral humeral attachment • scarred or weakened subscapularis muscle or tendon. • Neurovascular injury – musculocutaneous, axillary • Limitation of motion • Problems from retained hardware • Degenerative arthritis
Summary • Balance between the restoration of joint stability while minimizing loss of glenohumeral motion • Choice of treatment should be individualized • patient's occupation, level of participation in sports, degree of instability of the shoulder • No single "essential lesion" as proposed by Bankart • Bankart lesion is by far the most important • Open stabilization remains the standard procedure for treatment of anterior stabilization • esp. for severe instabilities, revision procedures, athletes in contact sports • Follow “anatomic repair principles”
Case • 25-year-old former collegiate football player presenting with 20 recurrent dislocations over the last 5 years
History • 25-year-old, right-hand-dominant, former collegiate football player • Suffered his first traumatic left shoulder dislocation at age 16 • He had an emergency room assisted reduction and was placed in a sling for 3 weeks • Underwent physical therapy for 2 months but subsequently had recurrent instability after returning to football • Age18, he underwent an arthroscopic Bankart reconstruction with 3 metal suture anchors • He began playing collegiate football, suffered a recurrent dislocation, and eventually had to discontinue playing • He has now had 20 recurrent dislocations over the last 5 years and presents for evaluation and treatment
Physical Examination • Active Shoulder Range of Motion: • Forward elevation180° bilaterally • ER (side) 60° bilaterally • ER (abduction) 90° bilaterally • IR T-7 spinous process bilaterally • Right Shoulder Instability Exam • Anterior load and shift 2+ • Posterior load and shift 1+ • Sulcus 1+ • Negative apprehension, relocation, anterior release • Left Shoulder Instability Examination: • Anterior load and shift 3+ • Posterior load and shift 1+ • Sulcus 1+ • No signs of generalized ligamentous laxity. • Positive apprehension, relocation, anterior release. • Normal neurological examination.
Imaging • Radiographs demonstrate a small Hill-Sachs lesion (yellow arrow) and the previously placed metal suture anchors (blue arrow).
Open anteroinferior capsular shift and Bankart procedure. • Modified beach chair position with the head elevated ~30° • Deltopectoral incision was used • Subscapularis was dissected off the underlying capsule
Bankart lesion • Capsule dissected off the humerus • Fukuda retractor placed to expose the glenohumeral joint • Large Bankart lesion was identified from the 6-9 o'clock position • Bioabsorbable suture anchors were used but had to be redirected carefully to avoid the previously placed metal suture anchors in the anteroinferior glenoid
Capsular Shift • Superolateral capsular shift (formal "T" capsulorrhaphy was not necessary) of the entire capsule • Arm placed in 30° abduction and 30° external rotation for capsular repair
Subscapularis Repair • Subscapularis was then anatomically repaired with #2 nonabsorbable sutures