Download
1 / 1
10 likes | 140 Views
Supporting & strengthening MNCH services using mobile phones: A research protocol. Frédérique Vallières & Eilish McAuliffe vallierf@tcd.ie. Phase I: Development of 7-11 into an open source mobile phone application

E N D
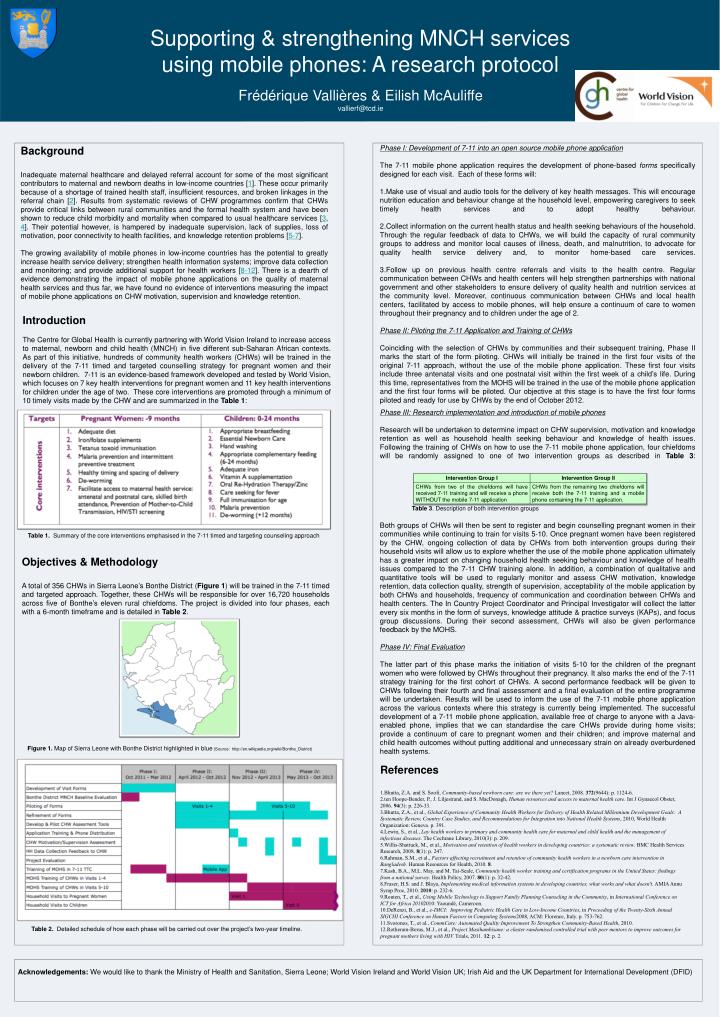
Supporting & strengthening MNCH services using mobile phones: A research protocol Frédérique Vallières & Eilish McAuliffe vallierf@tcd.ie • Phase I: Development of 7-11 into an open source mobile phone application • The 7-11 mobile phone application requires the development of phone-based forms specifically designed for each visit. Each of these forms will: • Make use of visual and audio tools for the delivery of key health messages. This will encourage nutrition education and behaviour change at the household level, empowering caregivers to seek timely health services and to adopt healthy behaviour. • Collect information on the current health status and health seeking behaviours of the household. Through the regular feedback of data to CHWs, we will build the capacity of rural community groups to address and monitor local causes of illness, death, and malnutrition, to advocate for quality health service delivery and, to monitor home-based care services. • Follow up on previous health centre referrals and visits to the health centre. Regular communication between CHWs and health centers will help strengthen partnerships with national government and other stakeholders to ensure delivery of quality health and nutrition services at the community level. Moreover, continuous communication between CHWs and local health centers, facilitated by access to mobile phones, will help ensure a continuum of care to women throughout their pregnancy and to children under the age of 2. • Phase II: Piloting the 7-11 Application and Training of CHWs • Coinciding with the selection of CHWs by communities and their subsequent training, Phase IImarks the start of the form piloting. CHWs will initially be trained in the first four visits of the original 7-11 approach, without the use of the mobile phone application. These first four visits include three antenatal visits and one postnatal visit within the first week of a child’s life. During this time, representatives from the MOHS will be trained in the use of the mobile phone application and the first four forms will be piloted. Our objective at this stage is to have the first four forms piloted and ready for use by CHWs by the end of October 2012. • Phase III: Research implementation and introduction of mobile phones • Research will be undertaken to determine impact on CHW supervision, motivation and knowledge retention as well as household health seeking behaviour and knowledge of health issues. Following the training of CHWs on how to use the 7-11 mobile phone application, four chiefdoms will be randomly assigned to one of two intervention groups as described in Table 3: • Table 3. Description of both intervention groups • Both groups of CHWs will then be sent to register and begin counselling pregnant women in their communities while continuing to train for visits 5-10. Once pregnant women have been registered by the CHW, ongoing collection of data by CHWs from both intervention groups during their household visits will allow us to explore whether the use of the mobile phone application ultimately has a greater impact on changing household health seeking behaviour and knowledge of health issues compared to the 7-11 CHW training alone. In addition, a combination of qualitative and quantitative tools will be used to regularly monitor and assess CHW motivation, knowledge retention, data collection quality, strength of supervision, acceptability of the mobile application by both CHWs and households, frequency of communication and coordination between CHWs and health centers. The In Country Project Coordinator and Principal Investigator will collect the latter every six months in the form of surveys, knowledge attitude & practice surveys (KAPs), and focus group discussions. During their second assessment, CHWs will also be given performance feedback by the MOHS. • Phase IV: Final Evaluation • The latter part of this phase marks the initiation of visits 5-10 for the children of the pregnant women who were followed by CHWs throughout their pregnancy. It also marks the end of the 7-11 strategy training for the first cohort of CHWs. A second performance feedback will be given to CHWs following their fourth and final assessment and a final evaluation of the entire programme will be undertaken. Results will be used to inform the use of the 7-11 mobile phone application across the various contexts where this strategy is currently being implemented. The successful development of a 7-11 mobile phone application, available free of charge to anyone with a Java-enabled phone, implies that we can standardise the care CHWs provide during home visits; provide a continuum of care to pregnant women and their children; and improve maternal and child health outcomes without putting additional and unnecessary strain on already overburdened health systems. Background Inadequate maternal healthcare and delayed referral account for some of the most significant contributors to maternal and newborn deaths in low-income countries [1]. These occur primarily because of a shortage of trained health staff, insufficient resources, and broken linkages in the referral chain [2]. Results from systematic reviews of CHW programmes confirm that CHWs provide critical links between rural communities and the formal health system and have been shown to reduce child morbidity and mortality when compared to usual healthcare services [3, 4]. Their potential however, is hampered by inadequate supervision, lack of supplies, loss of motivation, poor connectivity to health facilities, and knowledge retention problems [5-7]. The growing availability of mobile phones in low-income countries has the potential to greatly increase health service delivery; strengthen health information systems; improve data collection and monitoring; and provide additional support for health workers [8-12]. There is a dearth of evidence demonstrating the impact of mobile phone applications on the quality of maternal health services and thus far, we have found no evidence of interventions measuring the impact of mobile phone applications on CHW motivation, supervision and knowledge retention. Introduction The Centre for Global Health is currently partnering with World Vision Ireland to increase access to maternal, newborn and child health (MNCH) in five different sub-Saharan African contexts. As part of this initiative, hundreds of community health workers (CHWs) will be trained in the delivery of the 7-11 timed and targeted counselling strategy for pregnant women and their newborn children. 7-11 is an evidence-based framework developed and tested by World Vision, which focuses on 7 key health interventions for pregnant women and 11 key health interventions for children under the age of two. These core interventions are promoted through a minimum of 10 timely visits made by the CHW and are summarized in the Table 1: Table 1. Summary of the core interventions emphasised in the 7-11 timed and targeting counseling approach Objectives & Methodology A total of 356 CHWs in Sierra Leone’s Bonthe District (Figure 1) will be trained in the 7-11 timed and targeted approach. Together, these CHWs will be responsible for over 16,720 households across five of Bonthe’s eleven rural chiefdoms. The project is divided into four phases, each with a 6-month timeframe and is detailed in Table 2. Figure 1. Map of Sierra Leone with Bonthe District highlighted in blue (Source: http://en.wikipedia.org/wiki/Bonthe_District) References Bhutta, Z.A. and S. Soofi, Community-based newborn care: are we there yet? Lancet, 2008. 372(9644): p. 1124-6. ten Hoope-Bender, P., J. Liljestrand, and S. MacDonagh, Human resources and access to maternal health care. Int J Gynaecol Obstet, 2006. 94(3): p. 226-33. Bhutta, Z.A., et al., Global Experience of Community Health Workers for Delivery of Health Related Millennium Development Goals: A Systematic Review, Country Case Studies, and Recommendations for Integration into National Health Systems, 2010, World Health Organization: Geneva. p. 391. Lewin, S., et al., Lay health workers in primary and community health care for maternal and child health and the management of infectious diseases. The Cochrane Library, 2010(3): p. 209. Willis-Shattuck, M., et al., Motivation and retention of health workers in developing countries: a systematic review. BMC Health Services Research, 2008. 8(1): p. 247. Rahman, S.M., et al., Factors affecting recruitment and retention of community health workers in a newborn care intervention in Bangladesh. Human Resources for Health, 2010. 8. Kash, B.A., M.L. May, and M. Tai-Seale, Community health worker training and certification programs in the United States: findings from a national survey. Health Policy, 2007. 80(1): p. 32-42. Fraser, H.S. and J. Blaya, Implementing medical information systems in developing countries, what works and what doesn't. AMIA Annu Symp Proc, 2010. 2010: p. 232-6. Routen, T., et al., Using Mobile Technology to Support Family Planning Counseling in the Community, in International Conference on ICT for Africa 20102010: Yaoundé, Cameroon. DeRenzi, B., et al., e-IMCI: Improving Pediatric Health Care in Low-Income Countries, in Proceeding of the Twenty-Sixth Annual SIGCHI Conference on Human Factors in Computing Systems2008, ACM: Florence, Italy. p. 753-762. Svoronos, T., et al., CommCare: Automated Quality Improvement To Strengthen Community-Based Health, 2010. Rotheram-Borus, M.J., et al., Project Masihambisane: a cluster randomised controlled trial with peer mentors to improve outcomes for pregnant mothers living with HIV. Trials, 2011. 12: p. 2. Table 2. Detailed schedule of how each phase will be carried out over the project’s two-year timeline. Acknowledgements: We would like to thank the Ministry of Health and Sanitation, Sierra Leone; World Vision Ireland and World Vision UK; Irish Aid and the UK Department for International Development (DFID)




![Progressive Enhancement & Mobile [HOW Interactive 2012]](https://cdn4.slideserve.com/7565332/progressive-enhancement-mobile-dt.jpg)
![Intro to Adaptive Web Design [edUi 2013]](https://cdn4.slideserve.com/7565487/intro-to-adaptive-web-design-dt.jpg)