Download
1 / 47
470 likes | 481 Views
HPV and STI. Palm Beach State College Lunch and Learn Lecture Series March 20, 2013 Dudley Brown, Jr., MD, MBA. Background. AA Pre-Med--Broward Community College (1993) BS in Psychology--University of Miami (1995) MD--University of Florida College of Medicine (1999)

E N D
HPV and STI • Palm Beach State College • Lunch and Learn Lecture Series • March 20, 2013 • Dudley Brown, Jr., MD, MBA
Background • AA Pre-Med--Broward Community College (1993) • BS in Psychology--University of Miami (1995) • MD--University of Florida College of Medicine (1999) • MBA--Northern Illinois University (2011) • Residency in Obstetrics and Gynecology--Cook County Hospital, Chicago, IL (Chief Resident) • Private Practice for 10 yrs (8+ yrs in IL) • Office locations: West Palm Beach and Jupiter • Surgeries and Deliveries at Good Samaritan and St Mary’s Medical Centers in WPB • Accepting New Patients • (561)357-6277 • www.tenetfloridaphysicianservices.com
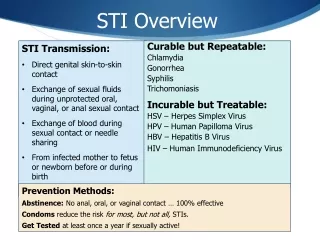
Human Papilloma Virus • Most common newly acquired sexually transmitted disease in the United States • An estimated 6.2 million new HPV infections occur each year • Currently 20 million people in the US are infected • Worldwide 630 million people are infected
Epidemiology of HPV • Double stranded DNA virus • Only infects humans • More than 100 types of HPV • Cutaneous and Mucous membranes
Human Papilloma Virus • 75% percent of sexually active Americans will be infected with HPV at some point in their lives • 74% percent of new cases occurs in individuals 15-24 years of age • Highest incidence consistently found in sexually active women younger than 25
Sexual Behaviors of High School Students • Survey of high school students reveal that 7.4% of students who responded reported having initiated sexual intercourse before 13 years of age • 22% of 9th graders • 49% of 12th graders
HPV Studies • Studies of adolescent and college-age women revealed that as many as 90% have tested positive for HPV at least 1 time • For males studies have revealed 30%. This lower number reflects the difficulty of detecting the virus in males
HPV Facts • Most individuals infected with HPV do not know that they are infected because they have no detectable HPV associated disease • Among adolescents the average HPV infection lasts a median of 5 to 6 months • Approximately 70% to 91% of HPV infections will regress within 2 years although the high risk types are more persistent
Prevalence of Cervical HPV Prevalence decreases sharply in women after age of 30 Those with persistent infection are at the highest risk for the development of high-grade precancerous lesions of invasive cervical cancer HPV testing in women 30 and older has been approved done along with a Pap smear
Diseases Caused by HPV • Cervical Cancer and Pre-cancerous cells • Vulva Cancer and Vaginal Cancer • Anal Cancer and Penile Cancer • Genital Warts( condyloma acuminatum) • Head and Neck Cancers • Recurrent Respiratory Papillomatosis
Transmission of HPV • HPV is spread primarily by sexual contact • Spread from mother to child at childbirth • Transmitted by non-penetrative sexual contact • Non-penetrative sexual contact includes finger-vulva, penile-vulva, oral-penile. • One study revealed that 10% of virgins had HPV infections
Risk Factors for HPV • High number of sexual partners • Previous infection with herpes simplex virus and other sexually transmitted diseases • Young age at initiation of sexual activity • HIV • Depressed immune system • Post-organ transplant such as kidney transplant
Types of HPV • There are over 100 types of HPV viruses • Of the 100 types only approximately 35 have been shown to infect the genital tract • Classified as high risk and low risk types • Risk of cancer is higher in the high risk types and lowest in the low risk types
Genotypes of HPV Low risks : 6 and 11, others 40,42,43,53,54,61,72,73 and 81 High risks: 16 and 18, others 31,33,35,39,45,51,52,58,59, and 68 Based on oncogenic (cancer) potential
Low Risk HPV • Genital Warts • Recurrent respiratory papillomatosis (mother to child) • Squamous intraepithelial lesions/ Abnormal Pap
Low Risk HPV • Types 6 and 11 • These types cause 90% of genital warts
High Risk HPV • Cervical Cancer & Pre-cancerous cells (Abn Pap) • Vulva Cancer • Vaginal Cancer • Anal Cancer • Penile Cancer • Head and Neck Cancers
High Risk HPV • Types 16 and 18 • These types cause 70% of cervical cancers • HPV 16 causes 60% of cervical cancers and HPV 18 causes 10% of cervical cancers Lancet Oncology 2010; 11:1048
High risk HPV • Persistent viral infection with high-risk HPV genotypes causes virtually all cancers of the cervix. • The same HPV types that cause cancer of the cervix also cause most cases of anal cancer. Hoots BE et al. Int J Cancer 2009;124:2375
Abnormal Paps • Low risk type will tend to resolve spontaneously without treatment • Approximately 10% - 13% will progress to higher grade lesions • High grade lesions have been shown to develop into cancer within 3 years if not treated
Cervical Cancer • Is the second most common cancer in women worldwide • Estimated 400,000 – 500,000 cases occur each year with 80% occurring in developing countries • In 2006 the American Cancer society estimated 9710 new cases with 3700 deaths in the United States
Medical Costs • In 2000 the direct medical costs of HPV infections among persons age 15 – 24 were estimated to total $2.9 billion dollars • False positive paps cost $350 million • Annual cervical screening cost $2.3 billion • Direct medical costs of abnormal paps with treatment is approximately $ 4.6 billion per year
Prevention of HPV • Abstinence • Condoms by 70% • Vaccine
HPV Vaccine June 8, 2006 the US Food and Drug Administration ( FDA )approved the HPV vaccine for use among females 9 to 26 years of age
Available HPV Vaccines • Gardasil, a quadrivalent vaccine, targets HPV types 6,11,16, and 18 • Cervarix, a bivalent vaccine, targets HPV types 16 and 18
HPV Vaccine Trials • Randomized double-blinded clinical trials of both vaccines were designed to determine if HPV immunization could prevent the development of cervical intraepithelial neoplasia (CIN2/3), adenocarinoma in situ,or cervical cancer related to HPV 16 and 18
Gardasil Vaccine Trials • 17,000 adolescents and young women • Among HPV negative, the efficacy of this quadrivalent vaccine for preventing CIN 2 or more severe disease due to HPV types included in the vaccine was 97 to 100 percent. • Among all trial participants ( with or without prior HPV infection), the efficacy was 44 percent. This reduction of efficacy in this group reflects the fact that the vast majority of enrollees in this trial were already sexually active and many had been previously infected with HPV
Cervarix Vaccine Trials • Trial enrolled 18,000 adolescents and young women • HPV negative group overall efficacy was 93% • Overall population of study participant efficacy was 30% • These data are consistent with those seen with the Gardisil vaccine trials and emphasize the need to vaccinate individuals before the onset of sexual activity to gain the greatest benefits N Engl J Med 2007; 356: 1928
HPV Vaccines • Vaccines are widely available in the Australia, Canada, Europe, and the United States for the prevention of cervical intraepithelial neoplasia and cervical cancer in women: in 2010, the FDA also approved this vaccine for the prevention of anal intraepithelial neoplasia and anal cancer in women based on the clinical trial results in men
Timing of immunization • Immunization with HPV is most effective among individuals who have not been infected with HPV • Approved for ages 9 to 26 • Optimal timing is before sexual activity • Females who are sexually active should be vaccinated up to target age of 26 • A history of abnormal Pap test, genital warts, or HPV infection is not a contraindication for the vaccine • However immunization is less beneficial for females who have already been infected with one or more of the HPV vaccines types
Serologic testing • Serologic testing or HPV DNA is not required prior to immunization
Recommendation for women • Advisory Committee on Immunization Practices (ACIP) has recommended that HPV vaccination be routinely offered to females between the ages of 11 and 12 years. Vaccine can be administered as early as age 9. Catch up vaccination is recommended for females aged 13 to 26 years who have not been previously vaccinated or who have not completed their vaccine series. • The American College of Obstetrics and Gynecologists (ACOG) follows the same recommendations
Recommendation for Males • Advisory Committee on Immunization Practices (ACIP) recommends HPV vaccine in males age 11 and 12. It can be given as early as age 9. Catch-up vaccination age 13 to 21 years • Permissive use of the vaccine in male age 22 to 26 • Permissive use means that the vaccine is recommended but not considered to be sufficient priority to include on a routine vaccination schedules • Vaccines recommended on a permissive basis is less likely to be covered by patient’s health insurance
Vaccine in Pregnancy • Although neither HPV vaccine contains no live virus, use in pregnancy is not recommended because of limited data on safety. • In the vaccine trials pregnancy occurred in 1053 women who started the series and no obvious fetal anomalies were observed. • In women who start the series and become pregnant before completion of all three shots, may resume the series in the postpartum period • Lactating women can receive the vaccine
HIV and Immunocompromised • HPV is not specifically recommended for persons with HIV infection, immunosuppression, or other chronic medical diseases. However according to ACIP guidelines its use can be considered since it is not a live vaccine.
Gardasil and Cervarix • Vaccination consists of a series of 3 shots • Gardasil Injections will be given at 0 months, 2 months, and 6 months followup • Cervarix injections will be given at 0 months, 1 months, and 6 months • Cost $120.00 per shot • Total of $360.00 for complete series • Many teens are eligible for free vaccination under the Vaccine for Children Program
CDC recommends when the series is interrupted for any length of time, it can resumed without restarting the series • Duration of protection- is unknown: to date women have been protected during a mean follow-up for 42 months Cancer Prev Res(Phila) 2009; 2;868
Side effects of Vaccine • Minimal • Most common: pain, swelling, and redness at injection site 1-2 days • Least common: fatique, headache, rash and upset stomach and temperature elevation
Adverse Reactions • In the United States, adverse events following immunizations are collected and analyzed within the Vaccine Adverse Event Reporting System (VAERS) • This data was compiled following administration of of approximately 40 million doses of HPV vaccines • From June 1, 2006 to September 2011, VAERS received 20,096 reports of adverse events following HPV immunization, 19,075 reports among females and 569 among males • Majority were mild 92% and 8 % serious including 72 deaths, of which 34 were confirmed. There was no unusual pattern or clustering to the deaths that would suggest that they were caused by the vaccine CDC Vaccine Safety/Vaccines/HPV assessed on November, 15,2011
Vaccine Adverse Event Reporting System • Most of the adverse reaction was not greater than those reported with other vaccines, with the exception of syncope and venous thromboembolic events, as detailed in a 2008 report. • Among 1896 syncopal reports , 15 % resulted in a fall or injury • Among the 31 with thromboembolism, 28(90%) had a known risk factor( estogen-containing birth control pills or a family history of clotting disorder). There were 4 deaths among the pulmonary embolism cases • Anaphylaxis has been reported. The over all risk rate of anaphylaxis in the VAERS is .1 case per 100,000 doses.
Advisory Committee on Immunization Practices • ACIP recommends a routine 15 minutes waiting period following vaccination so that the patient may continue in a sitting or supine position as needed; this may decease the risk of syncope with subsequent injury. • The rate of thrombotic events following HPV vaccination was not increased among those without prediposing risk factors
Cervical Cancer Screening • Cervical cancer screening with Pap test has reduced the incidence and mortality of cervical cancer by 70% over the past six decades. • Cervical cancer screening continues to be of great importance since HPV immunization will not prevent approximately 25-30% of cervical cancers in HPV negative and does not protect women already infected with carcinogenic HPV types against the development of cancer.
Conclusion • Vaccination against the most common types of HPV causing disease is expected to dramatically reduce the burden of illness associated with HPV. • Routine Pap smear screening is the best way to detect pre-cancerous cells and prevent cervical cancer • Dr Dudley Brown, Jr • Accepting New Patients (561)357-6277