Download
1 / 43
450 likes | 680 Views
Rational use of drugs: an overview. Kathleen Holloway Technical Briefing Seminar November 2009. Department of Essential Medicines and Pharmaceutical Policy TBS 2009. Objectives. Define rational use of medicines and identify the magnitude of the problem

E N D
Rational use of drugs:an overview Kathleen Holloway Technical Briefing SeminarNovember 2009 Department of Essential Medicines and Pharmaceutical Policy TBS 2009
Objectives • Define rational use of medicines and identify the magnitude of the problem • Understand the reasons underlying irrational use • Discuss strategies and interventions to promote rational use of medicines • Discuss the role of government, NGOs, donors and WHO in solving drug use problems
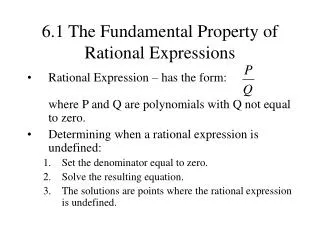
The rational use of drugs requires that patients receive medications appropriate to their clinical needs, in doses that meet their own individual requirements for an adequate period of time, and at the lowest cost to them and their community.WHO conference of experts Nairobi 1985 • correct drug • appropriate indication • appropriate drug considering efficacy, safety, suitability for the patient, and cost • appropriate dosage, administration, duration • no contraindications • correct dispensing, including appropriate information for patients • patient adherence to treatment
Adequacy of diagnostic processSource: Thaver et al SSM 1998, Guyon et al WHO Bull 1994, Krause et al TMIH 1998, Bitran HPP 1995, Bjork et al HPP 1992, Kanji et al HPP 1995.
5-55% of PHC patients receive injections - 90% may be medically unnecessary Source: Quick et al, 1997, Managing Drug Supply • 15 billion injections per year globally • half are with unsterilized needle/syringe • 2.3-4.7 million infections of hepatitis B/C and up to 160,000 infections of HIV per year associated with injections % of primary care patients receiving injections
Variation in outpatient antibiotic use in 26 European countries in 2002 Source: Goosens et al, Lancet, 2005; 365: 579-587; ESAC project.
Database on medicines use • Database of all medicines use surveys using standard indicators in primary care in developing and transitional countries • Studies identified from INRUD biliog, PUBMED, WHO archives • Data on study setting, interventions, methods and drug use extracted & entered • All data extraction and entry checked by 2 persons • Now > 900 studies entered • Systematic quantitative review • Evidence from analysis used for WHA60.16 in 2007
Public / private treatment of acute diarrhoea by doctors, nurses, paramedical staff
Overuse and misuse of antimicrobials contributes to antimicrobial resistance Source: WHO country data 2000-3 • Malaria • choroquine resistance in 81/92 countries • Tuberculosis • 0-17 % primary multi-drug resistance • HIV/AIDS • 0-25 % primary resistance to at least one anti-retroviral • Gonorrhoea • 5-98 % penicillin resistance in N. gonorrhoeae • Pneumonia and bacterial meningitis • 0-70 % penicillin resistance in S. pneumoniae • Diarrhoea: shigellosis • 10-90% ampicillin resistance, 5-95% cotrimoxazole resistance • Hospital infections • 0-70% S. Aureus resistance to all penicillins & cephalosporins
Community surveillance of AMR and use (1) • Developing & piloting method for integrated surveillance of AMR & AB use & collection of baseline data in 2 resource-constrained settings • 3 sites in India & 2 in S. Africa • AMR & AB use data collected monthly for 1-2 years from same communities • 4 sites measured AMR in E.Coli & 1 in S.pneum & H.influenzae • AB use by private GPs, retailers, public & priv hospitals & PHCs by exiting patient interview or prescribing & dispensing records • Qualitative study (FGDs) into provider & consumer behaviour
Community surveillance of AMR and use (2):results • Antimicrobial resistance • pathogenic E.Coli in pregnant women's urine in India • Cotrim 46-65%; Ampi 52-85%; Cipro 32-59%; Cefalex 16-50% • S.Pneumoniae & H.influenzae in sputa in S. Africa • Cotrim > 50% (both organisms); Ampi >70% (H.influenzae) • Antibiotic use • About ½ patients in India & ¼ or less of patients in S.Africa get ABs • Much inappropriate AB use especially in India e.g. use of fluoroquinolones for coughs and colds in private sector • Motivation of providers & consumers • Patient demand – looking for quick cure • Lack of CME & unwillingness to attend for fear of losing custom • Uncontrolled pharmaceutical promotion, involving financial gain
Adverse drug events Source: Review by White et al, Pharmacoeconomics, 1999, 15(5):445-458 • 4-6th leading cause of death in the USA • estimated costs from drug-related morbidity & mortality 30 million-130 billion US$ in the USA • 4-6% of hospitalisations in the USA & Australia • commonest, costliest events include bleeding, cardiac arrhythmia, confusion, diarrhoea, fever, hypotension, itching, vomiting, rash, renal failure
1. EXAMINE Measure Existing Practices (Descriptive Quantitative Studies) improve diagnosis 4. FOLLOW UP 2. DIAGNOSE Measure Changes Identify Specific in Outcomes Problems and Causes (Quantitative and Qualitative (In-depth Quantitative Evaluation) and Qualitative Studies) improve 3. TREAT intervention Design and Implement Interventions (Collect Data to Measure Outcomes) Changing a Drug Use Problem:An Overview of the Process
Intrinsic Prior Knowledge Scientific Information Habits Information Social &Cultural Factors Influenceof Drug Industry Treatment Choices Societal Economic & Legal Factors Workload & Staffing Workplace Infra-structure Authority & Supervision Relationships With Peers Workgroup Many Factors Influence Use of Medicines
Educational: • Inform or persuade • Health providers • Consumers Managerial: • Guide clinical practice • Information systems/STGs • Drug supply / lab capacity Use of Medicines Economic: • Offer incentives • Institutions • Providers and patients Regulatory: • Restrict choices • Market or practice controls • Enforcement Strategies to Improve Use of Drugs
Educational StrategiesGoal: to inform or persuade • Training for Providers • Undergraduate education • Continuing in-service medical education (seminars, workshops) • Face-to-face persuasive outreach e.g. academic detailing • Clinical supervision or consultation • Printed Materials • Clinical literature and newsletters • Formularies or therapeutics manuals • Persuasive print materials • Media-Based Approaches • Posters • Audio tapes, plays • Radio, television
Pre Post Impact of Patient-Provider Discussion Groups on Injection Use in Indonesian PHC Facilities Source: Hadiyono et al, SSM, 1996, 42:1185 % Prescribing Injections 80 60 40 20 0 Intervention Control
Training for prescribersThe Guide to Good Prescribing • WHO has produced a Guide for Good Prescribing - a problem-based method • Developed by Groningen University in collaboration with 15 WHO offices and professionals from 30 countries • Field tested in 7 sites • Suitable for medical students, post grads, and nurses • widely translated and available on the WHO medicines website
Managerial strategies Goal:to structure or guide decisions • Changes in selection, procurement, distribution to ensure availability of essential drugs • Essential Drug Lists, morbidity-based quantification, kit systems • Strategies aimed at prescribers • targeted face-to-face supervision with audit, peer group monitoring, structured order forms, evidence-based standard treatment guidelines • Dispensing strategies • course of treatment packaging, labelling, generic substitution
RCT in Uganda of the effects of STGs, training and supervision on % of Px conforming to guidelines Source: Kafuko et al, UNICEF, 1996.
Economic strategies:Goal: to offer incentives to providers an consumers • Avoid perverse financial incentives • prescribers’ salaries from drug sales • insurance policies that reimburse non-essential drugs or incorrect doses • flat prescription fees that encourage polypharmacy by charging the same amount irrespective of number of drug items or quantity of each item
Pre-post with control study of an economic intervention (user fees) on prescribing quality in Nepal Source: Holloway, Gautam & Reeves, HPP, 2001
PHC prescribing with and without Bamako initiative in Nigeria Source: Scuzochukwu et al, HPP, 2002
Regulatory strategiesGoal: to restrict or limit decisions • Drug registration • Banning unsafe drugs - but beware unexpected results • substitution of a second inappropriate drug after banning a first inappropriate or unsafe drug • Regulating the use of different drugs to different levels of the health sector e.g. • licensing prescribers and drug outlets • scheduling drugs into prescription-only & over-the-counter • Regulating pharmaceutical promotional activities Only work if the regulations are enforced
Intervention impact: largest % change in any medicines use outcome measured in each study source: database on medicines use 2009
Seminar (both groups) District-wide monitoring (both groups) Interactive group discussion (IGC group only) Impact of multiple interventions on injection use in Indonesia Source: Long-term impact of small group interventions, Santoso et al., 1996
What national policies do countries have to promote rational use? Source: MOH Pharmaceutical policy surveys 2003 and 2007
Increase Decrease For Iceland, total data (including hospitals) are used Slide courtesy of Otto Cars, STRAMA, Sweden
Co-ordination programs and national campaigns For Iceland, total data (including hospitals) are used Slide courtesy of Otto Cars, STRAMA, Sweden
Why does irrational use continue? Very few countries regularly monitor drug use and implement effective nation-wide interventions - because… • they have insufficient funds or personnel? • they lack of awareness about the funds wasted through irrational use? • there is insufficient knowledge of concerning the cost-effectiveness of interventions?
What are we spending to promote rational use of medicines ? • Global sales of medicines 2002-3 (IMS): US$ 867 billion • Drug promotion costs in USA 2002-3: US$ >30 billion • Global WHO expenditure in 2002-3: US$ 2.3 billion • Essential Medicines expenditure 2% (of 2.3 billion) • Essential Medicines expenditure on promoting rational use of medicines 10% (of 2%) • WHO expenditure on promoting rational use of medicines 0.2% (of 2.3 billion)
2nd International Conference for Improving Use of Medicines, Chiang Mai, Thailand, 2004472 participants from 70 countries http://www.icium.org Recommendations for countries to: • Implement national medicines programmes to improve medicines use • Scale up successful interventions • Implement interventions to address community medicines use
WHO priorities • Resolution WHA60.16 • Urges Member States " to consider establishing and/or strengthening…a full national programme and/or multidisciplinary national body, involving civil society and professional bodies, to monitor and promote the rational use of medicines " • WHO to support countries to implement resolution • Continue to give technical advice to countries • Model EML and formulary • Training on promoting RUM in community, PHC, hospitals • Research to identify cost-effective interventions • Advocacy
Health systems with no national programs: • No coordinated action • No monitoring of use of medicines Situational analysis WHO facilitating multi-stakeholder action in countries Develop national plans of action Modify action plans Implement & evaluate national action plans using govt & local donor funds • Health systems with national programs: • Coordinated action • Regular monitoring of use of medicine
Health system rapid appraisal tool (1): structurefor national stakeholders to rapidly appraise their own health systems in order to develop evidence-based national plans of action • Introduction • How to use the tool (in workbook format) and carry out the assessment (preparation, data collection, analysis) • Systematic data collection using document review, key informant interviews and observation with triangulation of results • Key respondent questionnaires • MOH senior dept managers (incl. dept pharmacy, DRA), • national drug supply organisation, insurance organisation(s), • health training institutions, health professional organisations, • health facility staff and health facility survey • Data collation and analysis by component • Identify recommendations for each component • Cross-cutting analysis & presentation to govt & donors • Analysis across components, prioritisation and formulation of national recommendations (to be completed)
Health system rapid appraisal tool (2): components • Components • Medicines use surveys and activities • Medicines policy framework • Health system factors • Service delivery & human resources, insurance, drug supply, regulation, financial (dis)incentives • Specific technical areas for RUM • National program coordination, MTCs, EMLs, STGs, monitoring, provider & consumer education, independent medicines info, AMR • Data for each component • Taken from key informant questionnaires & health facility survey, identifying relevant data from coding system of questions • Analysis for each component • Compares actual practice against best practice, choosing solutions from a menu of interventions
Creating the WHO Essential Drugs Libraryto facilitate the work of national committees Evidence-based clinical guideline Summary of clinical guideline WHO Model Formulary Reasons for inclusion Systematic reviews Key references WHO Model List Cost: - per unit - per treatment - per month - per case prevented Quality information: - Basic quality tests - Internat. Pharmacopoea - Reference standards
WHO-sponsored training programmes • INRUD/MSH/WHO: Promoting the rational use of drugs • MSH/WHO: Drug and therapeutic committees • Groningen University, The Netherlands / WHO: Problem-based pharmacotherapy • Amsterdam University, The Netherlands / WHO: Promoting rational use of drugs in the community • Newcastle, Australia / WHO: Pharmaco-economics • Boston University, USA / WHO: Drug Policy Issues
Global monitoring and identifying effective strategies to promote rational use of medicines • WHO/EMP databases on drug use and policy • quantitative data on medicines use and interventions to improve medicines use from 1990 to present day • data from MOHs on pharmaceutical policies every 4 years – 1999, 2003, 2007 • ICIUM3 in 2011 • 3rd international conference on improving the use of medicines (ICIUM3) • Surveillance of antimicrobial use & resistance • method for community-based surveillance in poor settings • interventional approach for improving use in private sector
Conclusions • Irrational use of medicines is a very serious global public health problem. • Much is known about how to improve rational use of medicines but much more needs to be done • policy implementation at the national level • implementation and evaluation of more interventions, particularly managerial, economic and regulatory interventions • Rational use of medicines could be greatly improved if a fraction of the resources spent on medicines were spent on improving use.
ActivityDiscuss in groups the following questions • What should be the roles of: • government, • NGOs and donors, • WHO, in promoting the rational use of medicines?