Download
1 / 71
710 likes | 893 Views
Review of HIV Therapy. Ronald D. Wilcox MD FAAP Project Director / Principal Investigator, DAETC Assistant Professor of Internal Medicine and Pediatrics, LSUHSC. Disclaimer. The speaker receives funding for research from the following companies: Tibotec Pfizer Boeringer-Ingelheim

E N D
Review of HIV Therapy Ronald D. Wilcox MD FAAP Project Director / Principal Investigator, DAETC Assistant Professor of Internal Medicine and Pediatrics, LSUHSC
Disclaimer • The speaker receives funding for research from the following companies: • Tibotec • Pfizer • Boeringer-Ingelheim • GlaxoSmithKline • Bristol-Myers-Squibb • Merck
Objectives • Review the life cycle of the HIV virus • Review the current medications for treatment of HIV • Review the current recommendations for initiation of HAART • Review appropriate prophylaxis for OIs
Question • How familiar are you with the different classes of HIV medications? 1. Very familiar – know all 7 classes and most of the agents 2. Can name at least 5 classes 3. Can name at least 3 classes 4. Can name at least 1 class 5. Know none of the classes of medications
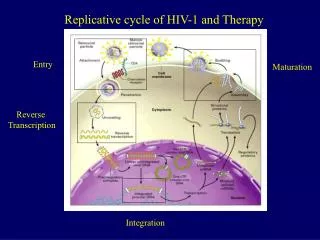
HIV Life Cycle • Attaches at CD4 marker with help of CXCR4 and CCR5 • Injects RNA into the cytoplasm • cDNA is made using reverse transcriptase • cDNA is integrated into the cell DNA using integrase and replication occurs • Protease cleaves the subsequent RNA and proteins into individual segments • Buds off or disrupts cell membrane for release
HAART Therapy • 4 major targets: • Fusion inhibition • CD4 receptor inhibitor • CCR5-Inhibitor • Reverse transcriptase enzyme • Nucleoside Reverse Transcriptase Inhibitors • Nucleotide Reverse Transcriptase Inhibitors • Non-Nucleoside Reverse Transcriptase Inhibitors • Integrase • Integrase Inhibitor • Protease enzyme • Protease inhibitors
Nucleoside RT Inhibitors • Abacavir (ABC) (1998) • Didanosine (ddI) (1991) • Emtricitabine (FTC) (2003) • Lamivudine (3TC) (1995) • Stavudine (d4T) (1994) • Zalcitabine (ddC) (1992) • Zidovudine (AZT, ZDV) (1987)
Case 1 • 28 year old obese patient is being seen by one of your colleagues. His current (second) HAART is d4T + Efavirenz + ddI and his viral load last month was < 400 on this regimen. He is also on dapsone for PcP prophylaxis. • The patient comes to your office complaining of some abdominal cramping over the past week that has steadily increased along with some nausea with one episode of emesis. No hematochezia, hematemesis, melena, diarrhaea, or constipation. He has also had lower extremity pain for 2 months.
Case 1 • Laboratory work-up reveals a WBC 8.2 with diff 66 s and 30 l. His H/H and platelets are within normal limits. His chemistry reveals a Na 128, K 3.4, Cl 98, CO2 14, BUN/Creat 22/1.4, glucose 88, and his AST and ALT are elevated at 2x the upper limits of normal. Lipase was 34.
Question • Which of the following is the most likely cause of the patient’s symptoms? • Methemoglobinemia from the dapsone • Pancreatitis from the ddI • Hepatitis from the efavirenz • Lactic acidosis from the d4T • Cryptosporidiosis of the gallbladder
Adverse Side Effect of Class • Lactic Acidosis + / - hepatic steatosis
Hepatic Steatosis / Lactic Acidosis • Mechanism: • Inhibitor of DNA polymerase gamma • (mitochondrial DNA synthesis) • Incidence: “Low” but with high fatality rate • Risk Factors: • Female sex, Obesity, Prolonged Use, Pregnancy • Presentation: • Non-specific GI (nausea, anorexia, pain, diarrhea), weakness, dyspnea, hepatomegaly, increased lactate, mild increase in transaminases, increased anion gap • Highest risk with d4T, esp when paired with ddI
Hepatic Steatosis / Lactic Acidosis • CT: SOME pts have enlarged, fatty liver • Screening: Do NOT stop RTI in every pt with lactate or transaminase elevation • Therapy: Stop RT if pt is symptomatic, acidotic, or lactate > 5 ? Riboflavin, Carnitine, Thiamine, Coenzyme Q • Rechallenge: Are any nucleosides safe?
Question • All of the following are considered examples of mitochondrial toxicity effects of nRTIs EXCEPT: 1. cardiomyopathy 2. pancreatitis 3. lipoatrophy 4. peripheral neuropathy 5. insulin resistance
Abacavir (ABC, Ziagen) • Pregnancy Risk Factor: C • Dosing: • 8 mg/kg BID up to 300 mg po BID • May give as 600 mg po daily • HYPERSENSITIVITY REACTION: • 2-8%; presents as anaphylaxis, fever, rash, fatigue, malaise, diarrhea, abdominal pain, N/V, respiratory symptoms, headache, myalgias/arthralgias • Screen with assay for HLA-B*5701 • Other ADEs: depression, dizziness, anxiety, thrombocytopenia, increased transaminases, myocardial infarction (90% increase)
Didanosine (ddI, Videx, Videx EC) • Pregnancy Risk Class: B • Comes as EC capsule or chewable tablets or liquid • Dosing: • Peds: 180-240 mg / m2 / day divided q12 • Adults: > 60 kg: 200 BID or 400 daily < 60 kg: 125 mg BID or 250 daily • MUST be on an EMPTY stomach (except when given with tenofovir) • Adverse side effect: Pancreatitis (2-3%), peripheral neuropathy (17-20%), retinal changes and optic neuritis, GI disturbances, increased transaminases and alkaline phosphatase, myocardial infarction (49% increase)
Emtricitabine (FTC, Emtriva) • Pregnancy Risk Class: B • Dosing: • Children > 33 kg and older: 200 mg daily with or without food • Children < 33 kg: 6 mg/kg/day (liquid) • Adverse Drug Effects: • Rash; Headache, dizziness, insomnia, diarrhea, nausea, weakness with increased CK, cough, abnormal dreams.
Lamivudine (3TC, Epivir) • Pregnancy Risk Class: C • Dosing: 150 mg bid or 300 mg daily • <50 kg: 2 mg/kg bid (liquid) • Adverse drug effects: • Well tolerated • Headache and fatigue > 10%, pancreatitis (higher in peds), peripheral neuropathy, neutropenia
Stavudine (d4T, Zerit) • Pregnancy Risk Class: C • Dosing: • Peds: 1 mg/kg bid (liquid) • Adults: <60 kg: 30 mg bid >60 kg: 40 mg bid • Adverse effects: • Peripheral neuropathy • Increased transaminases, triglycerides • Increased risk of lactic acidosis • Lipo-atrophy • Severe motor weakness
Zidovudine (AZT, ZDV, Retrovir) • Pregnancy Risk Class: C • Dosing: • 200 mg tid or 300 mg bid • Peds: 480 mg/m2 divided q6-q12 (liquid) • Postnatal: 2 mg/kg q6 x 6 weeks • Adverse drug effects: • Bone Marrow Suppression (23% anemia, 39% granulocytopenia in children)Myopathies • Headache (42%) GI Upset • Macrocytosis Bluish-brown Nails • Hair texture change in African-Americans
Combined Forms • Combivir: AZT + 3TC (1997) • Trizivir: AZT + 3TC + ABC (2000) • Truvada TDF + FTC (2004) • Epzicom ABC + 3TC (2004)
Nucleotide RT Inhibitors • Adefovir • Tenofovir (TDF) (2001)
Adefovir • No longer used in HIV care secondary to renal impairment
Tenofovir (TDF, Viread) • Pregnancy Risk Class: C • Dosing: • 300 mg daily • No peds dosing • Adverse drug effects: (equal to placebo) • Fanconi syndrome, renal insufficiency • Must change dosing with ClCr < 50 • 30-49: every 48 hours • 10-29: twice weekly • Hemodialysis: once weekly
Non-Nucleoside RT Inhibitors • Delavirdine (DLV) (1997) • Nevirapine (NVP) (1996) • Efavirenz (EFV) (1998) • Etravirine (ETV) (2008)
Delavirdine (DLV, Rescriptor) • Pregnancy Risk Class: C • Avoid use in lactating women • Dosing: (no peds dosing) • 400 mg tid or • 600 mg bid • Adverse drug effects: • Rash Elevated transaminases • Headache • Booster effect on some PIs: lopinavir, ritonavir, saquinavir
Nevirapine (NVP, Viramune) • Pregnancy Risk Class: B • Dosing: • 200 mg daily x 14 days then bid • (May give as 400 mg daily) • Peds: 120 mg/m2 bid (liquid) • Adverse Drug Effects: • RASH (15-20%) • Elevated transaminases – especially when used in PEP • Initiate cautiously with women with CD4 > 250 or men with CD4 > 400 • Neutropenia, diarrhea
Efavirenz (EFV, Sustiva) • Pregnancy Risk Class: D • Dosing: 600 mg qHS • Peds: based on weight {>10 kg} • Adverse Drug Effects: • CNS Stimulation:nightmares/abnormal dreams, dizziness, depression, anxiety, insomnia, jitteriness, daytime somnolence, psychosis, problems with memory and concentration • Rash (up to 46% in pediatrics) • Increased transaminases • Hyperlipidemia
Etravirine (TMC-125, Intelence) • Approved January 18, 2008 • Dosing: 100 mg (2) po BID • ADEs: rash (16.9%) and nausea (13.9%) • Salvage medication – must be used with a boosted protease inhibitor in the regimen
Protease Inhibitors • Amprenavir (1999) / fos-Amprenavir (fAMP) (2003) • Atazanavir (ATV) (2003) • Darunavir (DRV) (2006) • Indinavir (IND) (1996) • Lopinavir / rtv (LPV/r) (2000) • Nelfinavir (NLF) (1997) • Ritonavir (RTV) (1996) • Saquinavir (SQV) (1997) • Tipranavir (TPV) (2005)
Case 2 • 33 year old male patient presents to you office after being on d4T + ddI + Indinavir for 2 years with new complaints of increased urinary frequency and increasing fatigue. The patient reports that his shirt collar and pants are getting more tight and he reports concern about possible breast development.
Question • All of the following are metabolic side effects of the protease inhibitors EXCEPT: • Lipoatrophy • Lipodystrophy • Osteopenia • Insulin resistance • Hyperlipidemias
Case 2 • Laboratory work-up reveals: • Glucose 273 • UA with >1000 glucose • TG 875 with a total cholesterol of 266 • HDL 25
Insulin resistance • New onset DM or worsening of current DM • Insulin resistance • Impairment of glucose tolerance • Hyperglycemia • Frank diabetes rare
Lipid metabolism • Increase in triglycerides • Increase in cholesterol
Morphologic changes • Fat accumulation: • Abdominal obesity • Buffalo Hump • Lipomatosis • Breast enlargement
Lipoatrophy - nRTIs • Fat loss • Appendices • Face • Buttocks
Osteopenia • Highest incidence • Femoral head – osteonecrosis • Screen with DEXA scans
fos-Amprenavir (fAMP, Lexiva) • Pregnancy Risk Class: C • Dosing: • Unboosted: 1400 mg BID • Boosted Lexiva: 1400 mg with 100 mg Norvir daily (naive) OR 700 mg with 100 mg Norvir BID • Pediatric Dosing: (50 mg/ml) (2 years and older) • Unboosted: 30 mg/kg BID • Boosted: 18 mg/kg + Ritonavir 3 mg/kg BID • Adverse Drug Effects: • GI upset (N/V, diarrhea, taste disorders) • Rash • Circumoral paresthesias
Atazanavir (ATV, Reyataz) • Pregnancy Risk Class: B • Dosing: • PI-naïve patients: 200 mg (2) daily or ritonavir-boosted • PI-experienced patients: 300 mg daily with 100 mg Norvir • Adverse Drug Effects: hyperbilirubinemia, jaundice (5%) • Recent reports of kidney stones • PPI use – only in treatment-naïve patients on boosted atazanavir and given 12 hours apart • Cannot give with nevirapine
Darunavir (TMC-114, Prezista) • Pregnancy Risk Class: B • Dosing: • PI-experienced patients: 300 mg (2) or 600 mg (1) with 100 mg Norvir BID • Adverse Drug Effects: • Diarrhea, nausea & vomiting, headache, rash (7% and included all severities including Stevens-Johnson) • Elevated liver enzymes/hepatitis • Also perioral paresthesia, hepatitis, fat redistribution, hyperlipidemia, Type 2 diabetes are possible • Must take with food
Indinavir (IND, Crixivan) • Pregnancy Risk Class: C • Taken on empty stomach if given alone • Dosing: • Forms: 333 mg, 400 mg capsules • 800 mg q8 • Boosted – 800 mg bid with Norvir 100 mg with food • Peds: 500 mg/m2 q8 • Adverse Drug Effects: • NephrolithiasisHyperbilirubinemia • GI intolerance • 42-64 oz of fluids per day required • Best PI for CNS penetration studied
Lopinavir/RTV (LPV/r, Kaletra) • Pregnancy Risk Class: C • Dosing: • 400 mg/100 mg bid • 800 mg/200 mg po daily – naïve pts • 3 forms: tablets – 200 mg/50 mg tablets – 100mg/25 mg liquid – 5 cc • Adverse Drug Effects: • GI intolerance • Hyperlipidemias
Nelfinavir (NLF, Viracept) • Pregnancy Risk Class: B* • Must be taken after meals (500 kcal / 30% fat) • Dosing: • 250 mg or 625 mg tablets; 50 mg “scoops” • 750 mg tid OR 1250 mg bid • Peds: 20-30 mg/kg tid OR 50-55 mg/kg bid (mix with formula but avoid acidic juices) • Adverse Drug Effects: • DiarrheaRash • Weakness
Ritonavir (RTV, Norvir) • Pregnancy Risk Class: B • Dosing: • 600 mg bid • Booster effect: 100-200 mg bid • Taken with food • Store in refrigerator • Adverse drug effects: • GI Intolerance Taste Perversion • Circumoral, peripheral paresthesia • Elevated transaminases Fatigue
Saquinavir (SQV, Fortovase, Invirase) • Pregnancy Risk Class: B • Dosing: 500 mg tablets of Invirase • 1000 mg with Norvir 100 mg BID • 2000 mg with Norvir 100 mg Daily • No peds dosing • Adverse drug effects: • GI intolerance • Headaches • Elevated transaminases
Tipranavir (TPV, Aptivus) • Pregnancy Risk Class: B • Dosing: 250 mg tablets • 500 mg with Norvir 200 mg BID • No peds dosing • Cannot give with other PIs • Adverse drug effects: • GI intolerance Headaches • Elevated transaminases • Intracranial hemorrhages