Download
1 / 23
250 likes | 711 Views
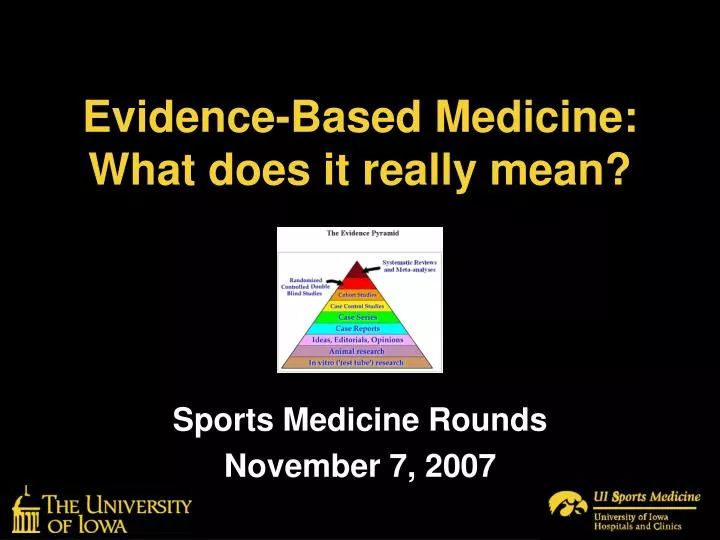
Evidence-Based Medicine: What does it really mean?. Sports Medicine Rounds November 7, 2007. What is Evidence-Based Medicine?. A Philosophical Framework? An Evolving Concept? A Method of Practice? A Quality Improvement Approach? A Teaching Tool?

E N D
Evidence-Based Medicine:What does it really mean? Sports Medicine Rounds November 7, 2007
What is Evidence-Based Medicine? • A Philosophical Framework? • An Evolving Concept? • A Method of Practice? • A Quality Improvement Approach? • A Teaching Tool? • A Potentially Dangerous Thing if used Incorrectly? ALL OF THE ABOVE
A New Concept? • The concept of modifying clinical practice based on research results has been in place for hundreds, perhaps thousands of years • In the 20th century (1990’s+) it has evolved to impact almost all fields of healthcare and policy; a structured approach
Largely Developed by One Group The specific methodologies used to determine “best evidence” were largely established by a research group led by David Sackett & Gordon Guyatt at McMaster U.
What is Evidence-Based Medicine? “Evidence-based medicine is the conscientious, explicit, & judicious use of current best evidence in making decisions about the care of individual patients” David Sackett, 1996
What is Evidence-Based Medicine? “The integration of best research evidence with clinical expertise & patient values” Sackett et al, 2000
Types of Evidence-Based Medicine • Evidence-based guidelines (EBG): practice of EBM at the organizational, institutional, or group level (establishing guidelines, policy, regulations)
Types of Evidence-Based Medicine • Evidence-based individual decision making (EBID): EBM as practiced by the individual healthcare provider in determining how to treat patients Some are suggesting we may be too EBM focused
Evidence-Based Medicine: A Process 1. Identify a patient-oriented/practice- oriented problem that is of interest 2. Develop a specific clinical question that targets the problem 3. Review the available evidence 4. Appraise the evidence → Decision 5. Integrate the evidence into your practice 6. Assess your outcomes (if appropriate)
An Idealistic EBM Model • Important not to confuse Levels of Evidence with Quality of Evidence or Importance
Study Design Should Match “?” • RCT: Homogeneous patients randomized to intervention A or B & compare outcomes • Longitudinal Cohort: Compare a group of people with a risk factor over time to see who develops a disease/injury; prognosis
Study Design Should Match “?” • Case-Control: People with condition are compared to those without on a set of variables to assess effect(s) or associations with variables; Diagnostic or descriptive • Cross-sectional Survey: A sample from a population is assessed for a certain disease/finding and specific risk factors at that single point in time; descriptive
Systematic Reviews & Meta-analyses • Systematic Review: • Structured review of the literature • Set inclusion & exclusion criteria • Assess study design quality • Assess methodological quality (rarely) • Compile & summarize results • Goal: determine what the current evidence is on a specific topic
Systematic Reviews & Meta-analyses • Meta-Analysis: • Also a structured review of the literature • Set inclusion & exclusion criteria • Assess study design quality • Assess methodological quality (rarely) • Perform statisticson the integrated results of the grouped studies • Goal: draw conclusions from the results of the analysis of the grouped data
Systematic Reviews • Goal: Summaries of best evidence; information overload • Top level of evidence; everyone doing them • Most are fair in terms of value • Over 1.3 Million listed in MEDLINE alone • About 5000 on the knee alone • Need to evaluate carefully
Systematic Review Killers • Low level research / Lack of Research • Heterogeneity of subject pools • Heterogeneity of methodology • Lack of detail prohibits comparison • Authors are often knowledgeable on general topic & evaluating study design & sources of bias, but not intervention methods
Must be Savvy Consumers of the Scientific Literature • Cannot just read abstract, conclusions, & look at figures • Hypotheses, methods, & results are most important • Design appropriate? • Bias? • Conclusion based on results & consistent with methods?
Things to Consider • EBM is only as good as the data available • A quality case-control study is more meaningful than a flawed RCT • Thus, systematic reviews of RCTs are not necessarily best evidence
Final Thoughts • Payers have also adopted this • Lack of evidence is being equated with lack of benefit; this is not true (call for evidence) • There are other clinical decision-making approaches • There are highly reputed health care experts who are stark opponents to the EBM approach accepted by most
Patient-Based Outcomes Measures • What do they tell us? • Does the KOOS QOL tell us someone’s knee is healthy? • Can it tell us how well someone is doing or does it simply tell us if there is noteworthy disability or not? • Is the difference between an 80 & 88 on the score the same as 88 to 96? • What is a good score? In a young athlete?