Download
1 / 79
810 likes | 852 Views
Learn about the different types of pleural diseases, including pleuritis, pneumothorax, and pleural effusions. Understand the causes, symptoms, diagnostic workup, and treatment options for each condition to help improve patient outcomes.

E N D
Pleural Disease pleuritis, pneumothorax & effusions
Pleuritis • Parietal pleura contains many pain fibers • Any inflammatory process can cause pain – “pleuritic pain” worse with deep breathing • Significance many times depends on clinical setting
19 y o college student Develops cough & congestion Similar to “ what’s going around “ Now has pain with deep inspiration 25 y o in third trimester of pregnancy Slipped on ice a few weeks ago & broke leg Has been on bedrest Now with SOB & pain with breathing Pleuritis cases
Pneumothorax • Entry of air into the pleural space – • can be a rent in the lungs from a biopsy or due to areas of gas trapping • compromise of the chest wall – air sucked in by negative pleural pressure • Symptoms depend on extent of pneumothorax & patient’s clinical status- air leaks usually last 72 hours
Tension Pneumothorax • A true medical emergency ! • Air escapes in to the pleura causing buildup of positive pressure in the thoracic cavity • May occur when patient on mechanical ventilation with air buildup causing compromise of venous return & shock • Patients need immediate decompression
Pneumothorax Causes • Iatrogenic – central lines, mechanical ventilation, lung biopsy • Abnormal lungs with areas of blebs, bullae - COPD • Abnormal airways with air-trapping due to ball-valve effect as with asthma • ARDS
21 y o center for BB team Has sudden onset of R sided chest pain & mild dyspnea Patient is uncomfortable but vital signs are WNL 20 y o severe asthmatic Intubated & on mechanical ventilation Suddenly becomes hypotensive & cyanotic Pneumothorax cases
Pleural Effusions Diagnostic workup
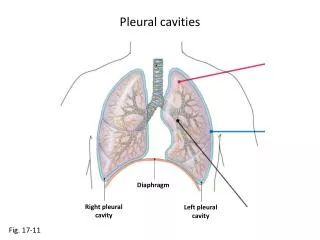
Radiographic signs of Pleural Effusion • Blunting of costophrenic angle on upright film • Elevation or flattening of hemi diaphragm on upright film • Diffuse haziness of hemi thorax on supine film • If large, will cause shift of mediastinum to contra-lateral side
Thoracentesis • Helpful diagnostically about 75% of the time • Can be therapeutic if the effusion is large & the patient is SOB at rest • Can safely remove up to 1500 cc of fluid • Especially if contralateral shift of mediastinum • Beware vague chest pain
Safe Tapping • Establish fluid is present & free flowing – Obtain lateral decubitus film – fluid level should be uniformly > 1 cm. or ID with U/S • Use ultrasound or CT to identify & locate loculated effusions • Experience decreases complications • Post-tap X-ray may not be necessary unless patient develops coughing, chest pain or dyspnea – PTX present < 1% with no symptoms
Relative Contraindications • Uncooperative patient • Bleeding diathesis, anticoagulation • Mechanical Ventilation esp. with high levels of PEEP • Too little fluid – beware of estimations based on CT appearance only
Diagnostic Thoracentesis - Tests • Studies to differentiate transudate from exudate : pleural fluid LDH, total protein & possibly albumin • Studies to help sort out an exudate: cell count & differential, glucose, cytology • Studies if warranted: Gram stain, AFB stain & culture, amylase, cholesterol, triglyceride level, pH, adenosine deaminase
Re-expansion Pulmonary Edema • Occurs when effusion present > 1 week • With drainage of > 1.5 L or no contralateral shift • Happens 1% thoracentesis with 20% mortality • Treatment is supportive – improves over 48-72 hours • Stop draining fluid if patient c/o SOB or vague chest pain
Therapeutic Thoracentesis • Can relieve sense of dyspnea: • Allows expansion of lung • Improves length – tension relationship of chest wall muscles & diaphragm • Creates more normal chest wall – lung working relationship • Degree of relief dependent on rapidity of accumulation & underlying condition of patient
What to do with the fluid ……. • Transudates: limited diagnostic possibilities & treatment options • Exudates: huge differential diagnosis & therapeutic options
Defining an Exudative Effusion • Ratio of pleural-fluid protein to serum protein > 0.5, pf cholesterol <45 • Ratio of pleural-fluid LDH > 0.6 • Pleural fluid LDH level > 60% upper limits of normal for serum or >200 • Any one of these characteristics means the fluid is an exudate • If exudate only by LDH likely parapneumonic or malignant
Transudates = ultra filtrate of serum • CHF – due to increased pulmonary venous pressures, usually bilateral, usually resolves in 48 hours after diuresis • Nephrosis – low oncotic pressures • Atelectasis – increased negative pleural pressure • Ascites – can preferentially form in pleural space, hepatic-hydrothorax
Pleural Effusion case #1 • 55 yo S/P large MI a few weeks ago • Presents now with DOE & orthopnea Chest X-ray shows enlarged heart with bilateral effusions R > than L. • Pleural fluid protein is 1.6, Serum protein is 5.8. Fluid LDH is 160, serum LDH is 420. • Echo shows LV ejection fraction of 20%
Albumin Gradient • Light’s criteria tend to overcall exudates • Especially in transudaive effusions after diuresis • If difference between albumin in serum minus pleural fluid is > 1.2 than more likely a true transudate • May misidentify 13%
Exudates: Diagnostic Dilemma • Mechanisms: • Increase permeability of pleural microcirculation due to inflammation • Impaired lymphatic drainage • Try to narrow down possibilities by using fluid characteristics
Large Exudative Effusions • Malignancy • Trauma - hemothorax • Empyema – bacterial infections • Chylothorax – disruption of thoracic duct • Rarely, TB
Exudative Effusions by Appearance • Bloody – cancer, pulmonary infarction, penetrating & nonpenetrating trauma, central line malplacement, chondrosarcoma, S/P CABG • Turbid – milky suggest chylothorax or gross pus equals empyema
Hemothorax • Defined as pleural fluid hematocrit of 50% of blood hematocrit • Will coagulate & may lead to loculation with complications of fibrothorax & possible empyema • If small, may defibrinate & remain free flowing
Exudative Effusions & Cell Count • > 50% lymphocytes – cancer, TB • > 10% eosinophils – blood or air in pleural space, drug reactions, asbestos exposure, paragonimiasis, early CABG, -does not rule out cancer • > 10% basophils – leukemic infiltration • > 50% neutrophils – acute process • > 5% mesothelial cells – TB less likely
Para pneumonic Effusion case • 46 y o with long Hx of ETOH abuse • Presents with low grade fever, weight loss & malaise • Physical exam is remarkable for poor dentition & decreased breath sounds on the right • Chest X-ray confirms moderately large pleural effusion
Case 2 cont. • Tap reveals a turbid odorous fluid with neutrophilic predominance • Just because, most of the specimens are lost • However the pH comes back at 6.9 • What to do next ??
Exudates & Bacterial Infections • Simple parapneumonic effusions are reactive to a pneumonia & resolve with antibiotics. Course is usually very benign • Empyemaor complicated parapneumonic effusions imply active bacterial infection in the pleural space. Failure to recognize & drain can lead to unresolved sepsis & fibro thorax
When to worry….. • Empyema means gross pus is present • Complicated parapneumonic effusion is defined by pH < 7.1 or glucose < 40 positive Gram stain or cultures • Borderline complicated is fluid with pH > 7.1 & < 7.2 or glucose > 40 or LDH > 1000 & Gram stain & cultures negative – needs RETAP
What to do ….. • Tube thoracostomy & antibiotics • Thrombolytics if loculated or stops draining despite fluid present on X-ray • Decortication if unable to achieve drainage & lung is trapped in fibrinous peel • Untreated may evolve to empyema necessitans or bronchopleural fistula causing overwhelming sepsis
Thrombolytics for drainage ? • May be helpful if coupled with DNAse • TPA alone – variable rate of success • Worth a shot if someone poor surgical risk • Instill and clamp tube for 2-4 hours • Dosing usually around 10 -20 mg x 3 days