Download
1 / 36
530 likes | 1.31k Views
Frontal Lobe Function and Dysfunction. Eric Ecklund -Johnson, Ph.D., ABPP(CN) ( eecklund-johnson@kumc.edu ) Clinical Neuropsychologist University of Kansas Hospital Center for Neuropsychology & Cognitive Neuroscience Clinical Assistant Professor University of Kansas Medical Center

E N D
Frontal Lobe Function and Dysfunction Eric Ecklund-Johnson, Ph.D., ABPP(CN) (eecklund-johnson@kumc.edu) Clinical Neuropsychologist University of Kansas Hospital Center for Neuropsychology & Cognitive Neuroscience Clinical Assistant Professor University of Kansas Medical Center Department of Neurology
Background • The human frontal lobes have been called the “organ of civilization” or similar names by such authorities as Ward Halstead and Alexander Luria and analogies have been made to a CEO, military general, orchestra conductor, etc. • Although it is no doubt an oversimplification, it is not entirely unreasonable to say that the frontal cortex and related structures allow what we think of as human personality to exist • The frontal lobes allow humans to think and plan beyond the present and rely less on instinct and more on reason than any other animal • Those who work with individuals who experience dysfunction of the frontal lobes and related structures are familiar with the sometimes profound changes in personality that can occur in addition to various higher-order cognitive deficits
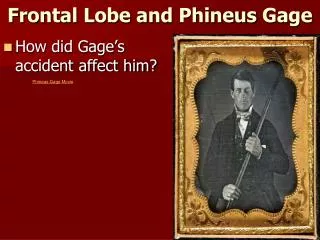
The Classic Case Study • The story of Phineas Gage is a classic and somewhat controversial case study of the potential impact of a certain type of frontal injury • Note, however, that there is disagreement regarding neuroscientists’ interpretations of Gage’s history (e.g., Kotowicz, 2007; Macmillan, 2002) • It is very likely that some accounts of his history have been exaggerated for effect to make (sometimes opposing) arguments, but his story is nevertheless of great interest to neuroscientists, particularly those who study frontal lobe function
Phineas Gage: The Basic Story • There are a number of well-established facts from first-hand accounts that are generally accepted by those who have studied Gage’s story • Gage was a Nineteenth Century railroad construction foreman who sustained an injury when an iron tamping rod was propelled through his skull, exiting through the top and traveling some distance • Gage amazingly survived the injury, returned to reasonably good physical health, and lived an additional 11 years, although he initially experienced a decline in alertness several days after the injury, presumed to have been due to brain swelling and also appears to have developed a subsequent brain infection • Accounts, particularly those of Harlow, the physician who attended to him, described a change in personality (Harlow, 1868), although the nature, extent, duration, and causes of this change are disputed
Phineas Gage: The Murkier History • Gage made at least one and perhaps several public appearances as a curiosity and kept the iron rod with him throughout the rest of his life • He also held a number of different jobs, moved several times, and later required assistance from his mother and sister as his health failed (including increasingly severe seizures near the end of his life) • He appears to have experienced personality change, was probably less responsible and more impulsive than in the past, and some (e.g., Damasio, 1995) have used his case to illustrate the contribution of the anterior frontal lobes to human ability to function in society • His treating physician (Harlow, 1868) stated “The equilibrium or balance, so to speak, between his intellectual faculties and animal propensities seems to have been destroyed” • However, MacMillan argues that Gage appears to have adjusted and become more functional over time (at least until near the end of his life), while Kotowicz argues that it may have been the disfigurement and not the brain injury itself that caused changes in personality/behavior
Phineas Gage: What has Subsequent Research Taught Us? • While the nature and extent of Gage’s personality changes are disputed, subsequent research leaves little doubt that damage to the frontal lobes, particularly certain regions, can cause marked alterations in behavior/personality • Research has suggested important regional differences within the frontal lobes that appear to result in meaningful distinctions in types of dysfunction (Malloy et al., 2006) • Recent work has also emphasized the connectivity of the frontal cortex and the important contributions of subcortical structures and other cortical regions to the complex functions typically attributed to the frontal lobes (e.g., Koziol et al., 2010) • Stuss (2006) describes interaction of the frontal lobes in a supervisory role with other regions of the brain and it appears that novel, complex tasks are much more likely to recruit frontal lobes than those that are well-learned and routine
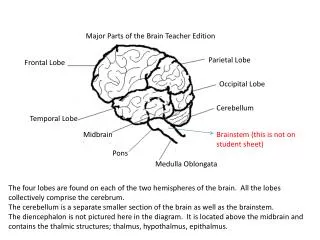
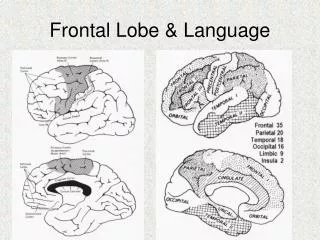
Anatomy • Frontal lobes encompass the territory anterior to the central sulcus (in front of parietal lobes) and superior to the temporal lobes • Broadly, frontal cortex can be divided (from posterior to anterior) into motor, premotor, and prefrontal regions, with limbic region primarily tucked under/within • There is hemispheric specialization, with the left frontal cortex involved in speech production and the right frontal cortex dominant perhaps for aspects of attention/awareness • Prefrontal cortex (anterior to motor/premotor areas) and frontal limbic cortex (medial and orbitofrontal aspects) are of special interest to psychologists, given their roles in cognition and emotion
Frontal Connections • As noted previously, frontal lobes are richly connected with other brain regions and most of these connections are bidirectional, observations which support their role in higher-order functions requiring integration of sensory, motor, and limbic information (Blumenfeld, 2002) • Cortical connections are primarily with association cortex (higher-order processing centers) of the parietal, occipital, and temporal (including connections with the amygdala and hippocampal formation in the temporal limbic cortex), lobes; also motor cortex and limbic cortex within the frontal lobes • Numerous connections with subcortical regions include (but are not limited to) several basal ganglia feedback ‘loops’, cerebellum, and areas within the thalamus
Areas Involved in Basal Ganglia ‘Loops’(from Blumenfeld, 2002)
Frontal Functions • Posterior frontal lobes are primary motor cortex – lesions here will produce paralysis or weakness on the contralateral side • Posterior/inferior (just above the temporal lobe) frontal lobe on the left side (assuming typical dominance) including Broca’s area is involved in speech production – lesions here will produce expressive aphasia • Prefrontal/limbic frontal cortex can be subdivided functionally into at least three zones (dorsolateral, orbitofrontal, medial), though specific functions may be less distinctly controlled by a particular frontal region than functions controlled primarily by other parts of the brain (Goldberg, 2002) and the greater the task complexity, the more likely that multiple zones will be recruited (Stuss, 2006)
Executive Functions • Term ‘executive function’ is often used synonymously with frontal function, but the two are not entirely overlapping and most tasks used to assess executive function also recruit areas outside of frontal cortex (Mesulam, 2000) • Functions typically labeled ‘executive’ include a broad range of higher functions with some of the most commonly described being cognitive set-shifting, inhibition of behavior, initiation, self-monitoring, planning, sequencing • Functional neuroimaging studies in the past 10-15 years have highlighted the fact that complex executive tasks are likely to recruit wide-ranging networks including multiple cortical and subcortical areas – this may often involve the frontal lobes playing a supervisory role
Frontal Syndromes • Malloy and colleagues (2006) suggest 3 major frontal syndromes (however, note that ‘pure’ examples may be uncommon clinically) • Dysexecutive (dorsolateral dysfunction): difficulty maintaining cognitive set, perseveration, cognitive rigidity, deficient self-monitoring, deficient working memory, deficient memory encoding/retrieval • Disinhibited (orbitofrontal dysfunction): impulsivity/disinhibition, social inappropriateness, stimulus-bound behavior, distractibility • Apathetic/Akinetic (medial dysfunction): decreased responsiveness to environment, reduced initiation, impersistence
Dysexecutive Syndrome • Early neuropsychological investigations (e.g., Milner, 1964) demonstrated difficulty shifting cognitive set, learning from errors, and generating words rapidly (i.e., verbal fluency) in the context of otherwise spared speech production were impaired in individuals with dorsolateral (but not orbital) frontal lesions, but not usually in individuals with other cortical lesions • Milner found that the way in which tasks were presented was important to demonstrating deficits in frontal patients – they were most likely to show greater difficulty when limited structure was provided • Subsequent research has generally supported the important contribution of the dorsolateral frontal cortex to such tasks, although again, functional imaging has demonstrated wide distribution of networks
Disinhibited Syndrome • Research suggests that damage to orbitofrontal and/or ventromedial cortex (anterior underside of frontal lobes) can cause personality/behavior changes often described as disinhibition, although risk-taking (as opposed to more general impulsivity) may be particularly affected (Floden et al., 2007) • A case that illustrates this syndrome dramatically (Burns & Swerdlow, 2003) involved an individual with a premorbidly controlled interest in pornography, but no known history of pedophilia who: • Developed impulsive sexual behavior including advances toward minors • This behavior resolved after resection of a right orbitofrontal tumor • The behavior again escalated a year later following tumor recurrence in the same location, and again resolved following re-resection
Apathetic/Akinetic Syndrome • Lesions in the medial frontal cortex involving anterior cingulate gyrus, particularly if bilateral, can result in reduced initiation/drive to the point of akinetic mutism (lack of spontaneous motor/speech behavior) if damage is extensive enough (Malloy et al., 2006). • If damage is more limited or only involves one side, akinetic mutism is usually transient, though more mildly reduced initiative may persist • Affect is typically flat and the person may appear to others to be depressed, although individuals with this syndrome often do not report subjectively depressed mood
Less Focal Frontal Signs/Symptoms • Frontal release signs include primitive reflexes (e.g., snout, grasp), though these reflexes are not highly specific and can be present in normal elderly (Malloy et al., 2006) • Environmental dependency– difficulty inhibiting the tendency to respond in a habitual way to environmental stimuli including utilization behavior (using objects in a non-goal directed manner) • Psychiatric syndromes such as reduplicative paramnesia (belief that a place has been duplicated) and Capgras syndrome (belief that a person has been duplicated) • Unawareness of deficits (Ecklund-Johnson & Torres, 2005; Schacter, 1990), though this may be more common with right frontal insult and can also be seen with non-frontal lesions such as in Wernicke’s aphasia
Common Disorders Affecting Frontal Function • There are numerous potential causes of frontal-system dysfunction, with some of the relatively more common ones including: • Frontotemporal dementia (e.g., Pick’s disease, others) • Neurodegenerative disease affecting interconnected structures (e.g., Parkinson’s disease) • Cerebrovascular disease (e.g., small vessel ischemia, ruptured anterior communicating artery aneurysm) • Traumatic brain injury • Tumor • Psychiatric conditions (e.g., schizophrenia, ADHD)
Frontotemporal Dementia • A gradually progressive neurodegenerative disease that occurs, on average, about 10 years earlier (median age of onset = 58) than is typical of (late-onset) Alzheimer’s disease (Kertesz, 2008) • Variable pathology can cause the clinical syndrome(s) of FTD, but Kertesz and others have emphasized the overlap, using the descriptor ‘Pick complex’ to describe the syndrome • There are really several syndromes, but often divided into ‘language variant’ and ‘behavioral variant’ with the latter representing the more classic ‘frontal’ presentation
Behavioral Variant FTD • The behavioral variant of FTD (bv-FTD) is characterized clinically by prominent early change in behavior/personality • Although symptoms of disinhibition/impulsivity are common and often striking, apathy/abulia (lack of initiative/spontaneous action) is even more common, especially later in the disease course (Mendez et al., 2008) • Theory of mind (ability to attribute mental states to oneself & others) appears to be impaired early in bv-FTD (Adenzato et al. 2010) and may contribute to impairment in appropriate social interaction and offensive or even aggressive behaviors that may occur
Behavioral Variant FTD • Insight/awareness of deficits is typically diminished early, usually to a greater extent than in early (though not necessarily later) stages of Alzheimer’s dementia • In many cases, the impaired insight may be more reflective of anosodiaphoria (emotional indifference toward the condition) than anosognosia (lack of awareness of deficits, Mendez et al. 2008) • Cognitive deficits are often much more subtle than behavioral changes early in the course of the disease and may go unrecognized, though thorough neuropsychological evaluation frequently (but certainly not always) reveals evidence of changes in executive functions
Other Neurodegenerative Disorders • Other neurodegenerative conditions, including several that affect primarily subcortical structures can cause a ‘subcortical/frontal’ syndrome • Parkinson’s disease primarily affects basal ganglia function and therefore has traditionally been thought of as primarily a motor disease; however, cognitive impairment and even dementia are common among patients with PD – perhaps up to ~50% or more at some point in the disease course (Buter et al., 2008) • Cognitive impairment in Parkinson’s disease typically includes prominent executive deficits in addition to slowed processing, visuospatial processing deficits, and inefficient memory encoding/retrieval with relatively preserved recognition (Tröster & Fields, 2008)
Other Neurodegenerative Disorders • The cognitive deficits have been associated with functional neuroimaging findings indicative of reduced metabolism in the basal ganglia and dorsolateral frontal lobes compared to controls (Tröster & Fields, 2008) • Other disorders that affect subcortical-frontal circuits and, in some cases frontal cortex, include Huntington’s disease, ‘Parkinson-plus’ syndromes (e.g., progressive supranuclear palsy, corticobasal ganglionic degeneration), Lewy-body dementia, and even essential tremor (possibly due to cerebellar-frontal disruption) • Demyelinating disorders such as multiple sclerosis often also present with a subcortical/frontal syndrome including executive deficits, slowed processing, and encoding/retrieval-based memory difficulty (Chelune et al. 2008)
Cerebrovascular Disease • Vascular dementia has been an evolving clinical concept associated with a fair amount of controversy • The previously prevailing concept of ‘multi-infarct’ dementia emphasized a relatively rare syndrome usually caused by >1 overt stroke, but more recent investigations suggest vascular dementia may be relatively common and does not require overt stroke (Brown et al. 2009) • More recently, the effects of vascular disease without overt stroke (‘lacunar’ infarcts and small vessel ischemic disease) have been increasingly of interest and have been associated with cognitive deficits (especially in executive functions and processing speed) in some, but certainly not all studies investigating them (Haaland & Swanda, 2008)
Cerebrovascular Disease • The degree to which small vessel ischemic disease alone can cause cognitive impairment remains controversial and white matter disease (presumed to be vascular) is ubiquitous in older adults who appear cognitively normal • Severe/extensive small vessel ischemia (‘Binswanger’s disease’) is likely sufficient in and of itself to cause a dementia syndrome; however, the pathological mechanism for this, though presumed to be vascular, is not fully understood (Haaland & Swanda, 2008) • In other cases, cerebrovascular disease may combine with neurodegenerative pathology to hasten a dementia syndrome or may cause a milder subcortical/frontal syndrome not sufficient to warrant a dementia diagnosis (i.e., ‘CIND’, Cato & Crosson, 2006)
Traumatic Brain Injury • Traumatic brain injury (TBI) can affect any brain region, but the frontal lobes, given their location and many connections, tend to be particularly vulnerable • Despite the media attention given to it, a single mild TBI (concussion) rarely causes substantial deficits for more than a brief period, whereas injuries defined as moderate or severe commonly produce lasting impairment that is correlated with injury severity at the group level (Dikmen & Machamer, 1995), though individual outcomes vary and are influenced by demographic variables (Goldstein et al., 2009) • Attention/processing speed, executive functions, and memory are most commonly impaired, while common emotional/behavioral changes include irritability, reduced insight, and reduced initiation (Roebuck-Spencer & Sherer, 2008), all of which can be associated with frontal dysfunction
Tumor • Tumors affecting the frontal lobes or interconnected structures can produce various frontal syndromes • In addition to location, aggressiveness and invasiveness of the tumor can be important factors in types of deficits seen and treatments (e.g., radiation, chemotherapy) can also introduce iatrogenic effects (Wefel et al., 2004) • Other issues, such as increased intracranial pressure due to swelling, seizures, etc. may also be present and contribute to symptoms • Any combination of the various frontal/executive syndromes described previously may be seen
Psychiatric Conditions • Psychologists generally understand that mind vs. brain/body distinctions present a false dichotomy and that psychiatric symptoms do not occur independently of brain function • Among the psychiatric conditions clearly linked to abnormal brain function, schizophrenia has attracted a good deal of research – while executive functions and attention are clearly among the most affected cognitive domains, verbal memory (but not necessarily forgetting) appears to be the most affected (Palmer et al., 2009) • While frontal structure/function is clearly affected, neuropathology of schizophrenia also extends well beyond the frontal lobes (Palmer et al., 2009)
Psychiatric Conditions • Some (e.g., Barkley, 1997) have proposed that deficits in executive function, presumably due to subcortical/frontal dysfunction, are the primary deficit in ADHD, although others (e.g., Willcut et al., 2005) argue that executive deficits, while common and important to the ADHD clinical picture, do not fully account for ADHD symptoms in all individuals • There is some evidence that psychopathy, at least in selected cases, may reflect a developmental insult to frontal (specifically, orbitofrontal) cortex (Anderson et al. 1999) • Depression with onset in late life has been associated with subcortical cerebrovascular disease of the type described previously (Alexopoulos et al, 1997; Potter et al., 2009)
Conclusion • The frontal lobes work closely with other areas of the brain, complicating claims of functions or syndromes as being uniquely ‘frontal’ • Nevertheless, the frontal lobes appear to be crucial to many of the abilities/behaviors that are unique to humans • Most human achievements rely heavily on such abilities as planning, inhibiting instinctive responses, and monitoring performance and would not be possible without the contribution of the frontal lobes
References Alexopoulis, G. S., Meyers, B. S., Young, R. C., Campbell, S., Silbersweig, D., Charlson, M. (1997). 'Vascular Depression' Hypothesis. Archives of General Psychiatry, 54, 915–922. Anderson, S. W., Bechara, A., Damasio, H., Tranel, D., & Damasio, A. R. (1999). Impairment of social and moral behavior related to early damage in human prefrontal cortex. Nature Neuroscience, 2(11), 1032-1037. Adenzato, M., Cavallo, M., & Enrici, I. (2010). Theory of mind ability in the behavioral variant of frontotemporal dementia: An analysis of the neural, cognitive, & social levels. Neuropsychologia, 48, 2-12. Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive function: Constructing a unified theory of ADHD. Psychological Bulletin, 121, 65-94. Blumenfeld, H. (2002). Neuroanatomy Through Clinical Cases. Sunderland, MA: Sinauer Associates. Brown, G. G., Lazar, R. M., & Delano-Wood, L. (2009). Cerebrovascular disease. In: I. Grant & K. M. Adams (Eds.): Neuropsychological Assessment of Neuropsychiatric and Neuromedical Disorders. New York: Oxford Press. Burns, J. M. & Swerdlow, R. H. (2003). Right orbitofrontal tumor with pedophilia symptom and constructional apraxia sign. Archives of Neurology, 60, 437-440. Buter, T. C., van den Hout, A., Matthews, F. E., Larsen, J. P., Brayne, C., & Aarsland, D. (2008). Dementia and survival in Parkinson disease: A 12-year population study. Neurology, 70,1017–1022.
Cato, M. A. & Crosson, B. A. (2006). Stable and slowly progressive dementias. In: D. K. Attix & K. A. Welsh-Bohmer (Eds.): Geriatric Neuropsychology: Assessment and Intervention. New York: Guilford Press. Chelune, G. J., Stott, H., & Pinkston, J. (2008). Multiple sclerosis. In: J. E. Morgan & J. H. Ricker (Eds.): Textbook of Clinical Neuropsychology. New York: Taylor & Francis. Damasio, A. (1995). Descartes’ Error: Emotion, Reason, and the Human Brain. New York: Penguin Putnam. Dikmen, S. & Machamer, J. (1995). Neurobehavioral outcomes and their determinants. Journal of Head Trauma Rehabilitation, 10, 74-86. Ecklund-Johnson, E. & Torres, I. (2005). Unawareness of deficits in alzheimer’s disease and other dementias: Operational definitions and empirical findings. Neuropsychology Review, 15(3), 147-166. Floden, D., Alexander, M. P., Kubu, C. S., Katz, D., & Stuss, D. T. (2007). Impulsivity and risk-taking behavior in focal frontal lobe lesions. Neuropsychologia, 46, 213–223 Goldberg, E. (2002). The Executive Brain: Frontal Lobes and the Civilized Mind. New York: Oxford Press. Goldstein, G., Allen, D. N., & Caponigro, J. M. (2010). A retrospective study of heterogeneity in neurocognitive profiles associated with traumatic brain injury. Brain Injury, 34(4), 625-635. Haaland, K. Y. & Swanda, R. M. (2008). Vascular dementia. In: J. E. Morgan & J. H. Ricker (Eds.): Textbook of Clinical Neuropsychology. New York: Taylor & Francis. Harlow, J. (1868). ‘Recovery from a Passage of an Iron Bar through the Head’, Publications of the Massachusetts Medical Society, 2, 327–47. Reprinted in Macmillan (2002).
Kertesz, A. (2008). Frontotemporal dementia: A topical overview. Cognitive and Behavioral Neurology, 21(3), 127-133. Kotowicz, Z. (2007). The strange case of Phineas Gage. History of the Human Sciences, 20, 115-131. Koziol, L. F., Budding, D. E., & Chidekel, D. (2010). Adaptation, expertise, and giftedness: towards an understanding of cortical, subcortical, and cerebellar network contributions. Cerebellum, 9(4), 499-529. MacMillan, M. (2002). An Odd Kind of Fame: Stories of Phineas Gage. London: MIT Press. Malloy, P. (2006). Frontal lobe function and dysfunction. In: P. J. Snyder, P. D. Nussbaum, & D. L. Robins (Eds.): Clinical Neuropsychology: A Pocket Handbook for Assessment. Washington DC: American Psychological Association. Mendez, M. F., Lauterbach, E. C., & Sampson, S. M. (2008). An evidence-based review of the psychopathology of frontotemporal dementia: A report of the ANPA Committee on Research. Journal of Neuropsychiatry & Clinical Neuroscience, 20(2), 130-149. Mesulam, M. M. (2000). Principles of Behavioral and Cognitive Neurology (2nd ed.). New York: Oxford Press. Milner, B. (1964). Some effects of frontal lobectomy in man. In: J.M. Warren & K. Akert (Eds.): The Frontal Granular Cortex and Behavior. New York: McGraw-Hill. Palmer, B. W., Dawes, S. E., & Heaton, R. K. (2009). What do we know about neuropsychological aspects of Schizophrenia? Neuropsychology Review, 19, 365–384.
Potter, G. G., McQuoid, D. R., Steffens, D. C., Welsh-Bohmer, K. A., & Krishnan, K. R. R. (2009). Neuropsychological correlates of magnetic resonance imaging-defined subcortical ischemic depression. International Journal of Geriatric Psychiatry 24, 219–225. Roebuck-Spencer, T. & Sherer, M. Moderate and severe traumatic brain injury. In: J. E. Morgan & J. H. Ricker (Eds.): Textbook of Clinical Neuropsychology. New York: Taylor & Francis. Schacter , D.L. (1990). Toward a cognitive neuropsychology of awareness: Implicit knowledge and anosognosia . Journal of Clinical and Experimental Neuropsychology, 12, 155 – 178. Stuss, D. T. (2006). Frontal lobes and attention: Processes and networks, fractionation and integration. Journal of the International Neuropsychological Society, 12, 261-271. Tröster, A. I. & Fields, J. A. (2008). Parkinson’s disease, progressive supranuclear palsy, corticobasal degeneration, and related disorders of the frontostriatal system. In: J. E. Morgan & J. H. Ricker (Eds.): Textbook of Clinical Neuropsychology. New York: Taylor & Francis. Wefel, J. S., Kayl, A. E., & Meyers, C. A. (2004). Neuropsychological dysfunction associated with cancer and cancer therapies: A conceptual review of an emerging target. British Journal of Cancer, 90,1691-1696. Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biological Psychiatry, 57, 1336-1346.