Download
1 / 2
20 likes | 159 Views
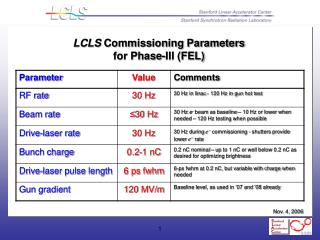
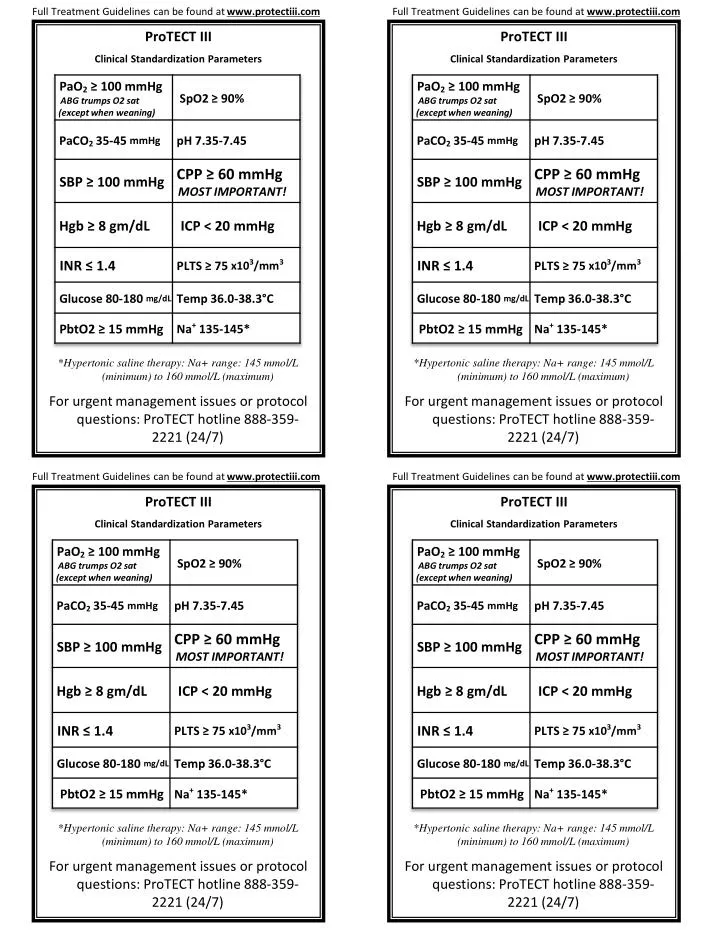
Full Treatment Guidelines can be found at www.protectiii.com. Full Treatment Guidelines can be found at www.protectiii.com. ProTECT III Clinical Standardization Parameters * Hypertonic saline therapy: Na+ range: 145 mmol/L (minimum) to 160 mmol/L (maximum)

E N D
Full Treatment Guidelines can be found at www.protectiii.com Full Treatment Guidelines can be found at www.protectiii.com ProTECT III Clinical Standardization Parameters *Hypertonic saline therapy: Na+ range: 145 mmol/L (minimum) to 160 mmol/L (maximum) For urgent management issues or protocol questions: ProTECT hotline 888-359-2221 (24/7) ProTECT III Clinical Standardization Parameters *Hypertonic saline therapy: Na+ range: 145 mmol/L (minimum) to 160 mmol/L (maximum) For urgent management issues or protocol questions: ProTECT hotline 888-359-2221 (24/7) Full Treatment Guidelines can be found at www.protectiii.com Full Treatment Guidelines can be found at www.protectiii.com ProTECT III Clinical Standardization Parameters *Hypertonic saline therapy: Na+ range: 145 mmol/L (minimum) to 160 mmol/L (maximum) For urgent management issues or protocol questions: ProTECT hotline 888-359-2221 (24/7) ProTECT III Clinical Standardization Parameters *Hypertonic saline therapy: Na+ range: 145 mmol/L (minimum) to 160 mmol/L (maximum) For urgent management issues or protocol questions: ProTECT hotline 888-359-2221 (24/7)
Full Treatment Guidelines can be found at www.protectiii.com Full Treatment Guidelines can be found at www.protectiii.com • Defer non-emergent surgeries until cleared by NeuroSurg • Please record GCS daily in progress note - list total score & each component (E, V, M) • Pressure Recommendations and Euvolemia: • Patients who are intubated or who have a ventriculostomy should have an art line and CVP monitor. • Use Normal Saline Fluid as initial method of maintaining euvolemia (CVP 5‐7 mmHg) to achieve target BP, followed by pressors. • CPP ≥ 60 mmHg should drive therapy • ICP Monitoring: Refer to ICP Tiers 1, 2, & 3 in chart • Consider all Tier 1 interventions first • Tier 1: Mannitol must be used before HTS • SpO2 > 90 % remains goal during active weaning of ventilation • Prophylactic hyperventilation (PaCO2 < 35 mmHg) is prohibited. • Coagulation: • Consider one or more: FFP, Vitamin K, DDAVP, prothrombin complex concentrate, or Factor VII as clinically indicated • Anemia: Blood should be transfused for Hgb <8 g/dL. • Antiseizure Prophylaxis: • Phenytoin or Fosphenytoin - obtain therapeutic levels per hospital policy • Do NOT use glucocorticoids as a treatment for TBI (ok for other conditions) • Defer non-emergent surgeries until cleared by NeuroSurg • Please record GCS daily in progress note - list total score & each component (E, V, M) • Pressure Recommendations and Euvolemia: • Patients who are intubated or who have a ventriculostomy should have an art line and CVP monitor. • Use Normal Saline Fluid as initial method of maintaining euvolemia (CVP 5‐7 mmHg) to achieve target BP, followed by pressors. • CPP ≥ 60 mmHg should drive therapy • ICP Monitoring: Refer to ICP Tiers 1, 2, & 3 in chart • Consider all Tier 1 interventions first • Tier 1: Mannitol must be used before HTS • SpO2 > 90 % remains goal during active weaning of ventilation • Prophylactic hyperventilation (PaCO2 < 35 mmHg) is prohibited. • Coagulation: • Consider one or more: FFP, Vitamin K, DDAVP, prothrombin complex concentrate, or Factor VII as clinically indicated • Anemia: Blood should be transfused for Hgb <8 g/dL. • Antiseizure Prophylaxis: • Phenytoin or Fosphenytoin - obtain therapeutic levels per hospital policy • Do NOT use glucocorticoids as a treatment for TBI (ok for other conditions) Full Treatment Guidelines can be found at www.protectiii.com Full Treatment Guidelines can be found at www.protectiii.com • Defer non-emergent surgeries until cleared by NeuroSurg • Please record GCS daily in progress note - list total score & each component (E, V, M) • Pressure Recommendations and Euvolemia: • Patients who are intubated or who have a ventriculostomy should have an art line and CVP monitor. • Use Normal Saline Fluid as initial method of maintaining euvolemia (CVP 5‐7 mmHg) to achieve target BP, followed by pressors. • CPP ≥ 60 mmHg should drive therapy • ICP Monitoring: Refer to ICP Tiers 1, 2, & 3 in chart • Consider all Tier 1 interventions first • Tier 1: Mannitol must be used before HTS • SpO2 > 90 % remains goal during active weaning of ventilation • Prophylactic hyperventilation (PaCO2 < 35 mmHg) is prohibited. • Coagulation: • Consider one or more: FFP, Vitamin K, DDAVP, prothrombin complex concentrate, or Factor VII as clinically indicated • Anemia: Blood should be transfused for Hgb <8 g/dL. • Antiseizure Prophylaxis: • Phenytoin or Fosphenytoin - obtain therapeutic levels per hospital policy • Do NOT use glucocorticoids as a treatment for TBI (ok for other conditions) • Defer non-emergent surgeries until cleared by NeuroSurg • Please record GCS daily in progress note - list total score & each component (E, V, M) • Pressure Recommendations and Euvolemia: • Patients who are intubated or who have a ventriculostomy should have an art line and CVP monitor. • Use Normal Saline Fluid as initial method of maintaining euvolemia (CVP 5‐7 mmHg) to achieve target BP, followed by pressors. • CPP ≥ 60 mmHg should drive therapy • ICP Monitoring: Refer to ICP Tiers 1, 2, & 3 in chart • Consider all Tier 1 interventions first • Tier 1: Mannitol must be used before HTS • SpO2 > 90 % remains goal during active weaning of ventilation • Prophylactic hyperventilation (PaCO2 < 35 mmHg) is prohibited. • Coagulation: • Consider one or more: FFP, Vitamin K, DDAVP, prothrombin complex concentrate, or Factor VII as clinically indicated • Anemia: Blood should be transfused for Hgb <8 g/dL. • Antiseizure Prophylaxis: • Phenytoin or Fosphenytoin - obtain therapeutic levels per hospital policy • Do NOT use glucocorticoids as a treatment for TBI (ok for other conditions)