Download
1 / 38
380 likes | 584 Views
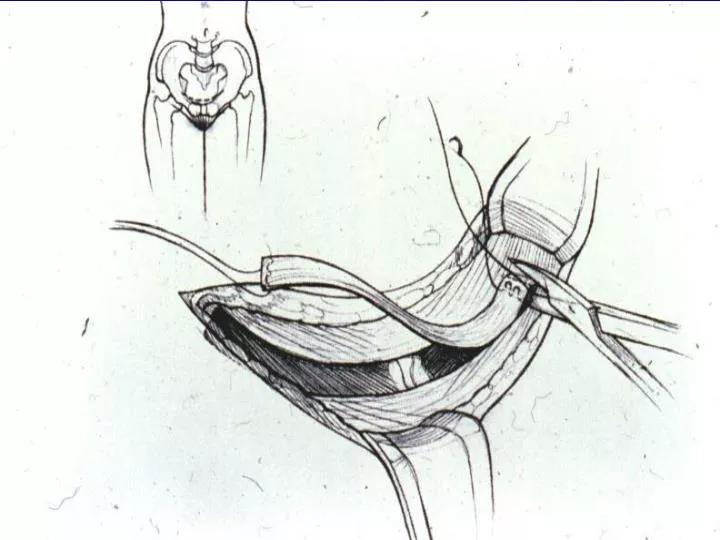
Cartoon of taking fascia. Surgical Technique. Horizontal suprapubic incision (4 cm) Excise rectus fascial strip (6 – 8 cm) Temporarily leave fascia open Horizontal incision over vesical neck. Surgical Technique. Mobilize vesical neck from below Perforate endopelvic fascia

E N D
Surgical Technique • Horizontal suprapubic incision (4 cm) • Excise rectus fascial strip (6 – 8 cm) • Temporarily leave fascia open • Horizontal incision over vesical neck
Surgical Technique • Mobilize vesical neck from below • Perforate endopelvic fascia • Create tunnel & pass slingaround vesical neck • Cystoscopy
Surgical Technique • Close vaginal wound • Bring sutures through fascia • Close rectus fascia • Suture ends of sling togetherin midline without tension • Close abdominal wound
Balloon Incision
Push up withindex finger onvaginalwall Traction ofclamp
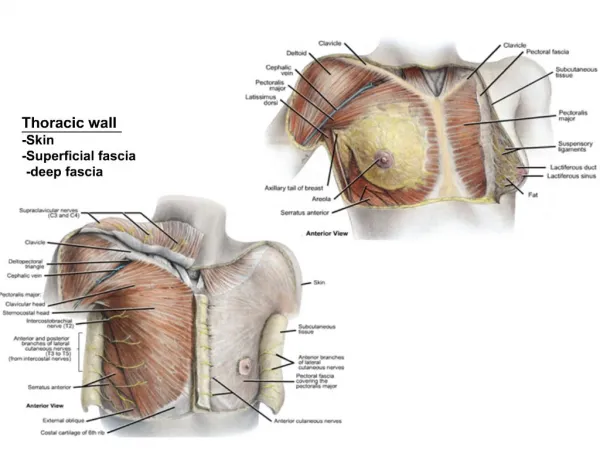
Left index finger pushing up on vaginal wall Shiny white surface superficialto pubo-cervical fascia
Incorrect (deep) plane Correct (superficial) plane
Correct (superficial) plane Pubo-cervical fascia Incorrect (deep) plane
Sutures through separate stabwounds in rectus fascia Ends of sling thru fascia
How much tension? • None (create a backboard) • (Almost) can’t make it too loose • Make sure Q-tip is not negative(elevation of vesical neck)
Take slack out ofsling Push down on cystoscope parallel to thefloor
PVS for Simple SUI OUTCOME SCORE 100% 0%
Mixed Incontinence • Cure/Improved Rates (UIOS <= 4) : • SUI: 97% (n= 44) • MUI: 93% (n= 47)non-significant difference (p: 0.33), with study powered a priori to detect > 20% difference in outcome score Chou et al, J Urol, 2003
Autologous Sling Outcomes • Cure/Improve rate - 82% at 4 years • Urinary Retention requiring intervention - 8% • De Novo OAB - 9% (Dmochowski, et al. AUA Guidelines on the Surgical Management of Female Stress Urinary Incontinence, 2010)