Download
1 / 47
480 likes | 822 Views
Pre-clinical Periodontics. Dr Jamal Naim PhD in Orthodontics. Classification of periodontal diseases. Definitions. Gingivitis and periodontitis are inflammatory diseases of bacterial origin.

E N D
Pre-clinical Periodontics Dr Jamal Naim PhD in Orthodontics Classification of periodontal diseases
Definitions Gingivitis and periodontitis are inflammatory diseases of bacterial origin. Gingivitis is completely reversible, but the destruction caused by periodontitis is partially reversible.
Gingivitis versus Periodontitis Early definitions: Gingivitis is inflammation limited to the gingivae in which the JE remains attached to the tooth at its original level and is completely reversible.
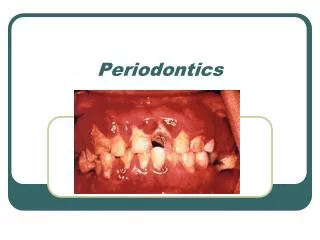
Gingivitis versus Periodontitis Mild gingivitis
Gingivitis versus Periodontitis If there is any destruction (attachment loss) in the tooth supporting tissues (PDL, Gingiva, alveolar bone), then we speak about periodontitis. According to these early definitions the presence of gingival inflammation in a patient with existing but not progressing attachment loss is also called periodontitis.
Gingivitis versus Periodontitis Periodontitis with attachment loss and infrabony pocket
Gingivitis versus Periodontitis Recent definitions: Gingivitis is the inflammation of a periodontium with no attachment loss or with previous attachment loss that is stable and not progressing. Periodontitis is the inflammation of a periodontium caused by specific microorganisms resulting in progressive destruction of the PDL and alveolar bone (attachment loss) with pocket formation, recession or both.
Classification of periodontal diseases • Gingivitis • Mild • Moderate • Severe • Acute Necrotizing Ulcerative • Modulated by hormones • Gingival overgrowth and etc. • Periodontitis • Adult Periodontitis • Rapidly progressive Periodontitis (RPP) • Localized juvenile Periodontitis (LJP) • ANUP
Classification of periodontal diseases EARLY CLASSIFICATIONS
EARLY CLASSIFICATIONS AAP until 1999 European workshop on Perio 1993
Classification of periodontal diseases The need for a revised classification system for periodontal diseases was emphasized during the 1996 World Workshop in Periodontics. In 1997 the American Academy of Periodontology (AAP) responded to this need and formed a committee to plan and organize an international workshop to revise the classification system for periodontal diseases. On October 30–November 2, 1999, the International Workshop for a classification of Periodontal Diseases and Conditions was held and a new classification was agreed upon
Classification of periodontal diseases • Gingival diseases: A. Dental plaque-induced gingival diseases • ? • ? • etc. B. Non-plaque-induced gingival lesions • ? • ? • etc.
Classification of periodontal diseases II. Chronic Periodontitis: A. Localized B. Generalized III. Aggressive Periodontitis: A. Localized B. Generalized
Classification of periodontal diseases IV. Periodontitis as a Manifestation of Systemic Diseases: A. Associated with hematological disorders B. Associated with genetic disorders C. Not otherwise specified (NOS) V. Necrotizing Periodontal Diseases: A. Necrotizing ulcerative gingivitis (NUG) B. Necrotizing ulcerative periodontitis (NUP)
Classification of periodontal diseases VI. Abscesses of the Periodontium: A. Gingival abscess B. Periodontal abscess C. Pericoronal abscess VII. Periodontitis Associated With Endodontic Lesions: A. Periodontic-endodontic lesions B. Endodontic-periodontic lesions C. Combined periodontic-endodontic lesions
Classification of periodontal diseases VIII. Developmental or Acquired Deformities and Conditions: A. Localized tooth-related factors that modify or predispose to plaque-induced gingival diseases/periodontitis B. Mucogingival deformities and conditions around teeth C. Mucogingival deformities and conditions on edentulous ridges D. Occlusal trauma
Pre-clinical Periodontics Dr Jamal Naim PhD in Orthodontics Etiology & pathogenesis of periodontal diseases
Cocci Rods Curved rods Spiral (spirochaetes) Bacteria exist in different shapes
Arrangement Bacteria arrange themselves as: • Pairs (diplococci) • Chains (streptococci) • Grape-like clusters (staphylococci)
Gram-staining characteristics Classified into two major subgroups: • Gram-positive (purple) • Gram-negative (pink) What for? • Bacteria identification • Therapy of bacterial infection
Origin of normal oral flora • Sterile until birth, bacteria acquired from birth canal from mother • Infant exposed to flora of mother, other people and organisms in the environment • Oral flora on the child’s first birthday usually consist of streptococci, staphylococci, lactobacillus, less frequently isolated actinomyces, prevotella, fusobacterium species
Origin of normal oral flora • The pioneer species are usually streptococci which bind to mucosal epithelium and remain throughout life • The metabolic activity of the pioneer community then alters the oral environment to facilitate colonization by other bacterial species.
Origin of normal oral flora • The next change in this community occurs during and after tooth eruption: • Hard tissue surface of enamel (s. mutans) • Gingival crevice (prevotella gingivalis) • A second childhood is reached if all teeth are lost. Bacteria are very similar to those in a child before tooth eruption. • Introduction of a prosthetic appliance at this stage changes the microbial composition once again. • Acrylic denture (Candida) • Over 70 y (Staphylococcus aureus, lactobacilli)
The oral ecosystem • The mouth has a natural microflora (commensal, indigenous, or resident) which exists in a harmony with the host, (like skin, Nasopharynx, Gastro-intestinal tract including oral cavity) • Commensal (resident) flora – fixed types of microbes regularly found in a given area at a given age
The oral ecosystem Commensal bacteria do not cause disease unless: • Resistance of the HOST is poor OR • Commensal bacteria are relocated to sites where they don’t usually live. • e.g. streptococci from mouth Upper respiratory tract entering blood stream after tooth extraction, scaling & toothbrushing can cause endocarditis.
The oral ecosystem • 600 species of commensal (resident) bacteria • an estimated 415 species present in subgingival plaque. • Fungi (yeasts) such as Candida albicans, • Viruses eg herpes, Epstein-Barr.
The oral ecosystem The nature of the site determines the type of bacteria. ie. interproximal, occlusal, supragingival, subgingival
The oral ecosystem • Transient flora – non-pathogenic or potentially pathogenic flora on skin or mucous membranes; derived from the environment & does not establish permanently. • Transient flora – of little significance as long as the normal resident flora remains in place.
The oral ecosystem Diverse habitats for bacteria: • tongue (provides the home for the majority of oral bacteria) • Mucosa (K, non-K) • teeth (non-shedding area) • gingival crevice, • saliva (contains up to 108 bacteria/ml), • tonsils. • Prosthodontic and orthodontic appliances
What is the ‘white stuff’ present on the labial surfaces of the lower anterior teeth? How does the white stuff form ? Does the white deposit cause any problems for the gums or teeth ? Why are the labial surfaces of the teeth partly brown ?
Dental Deposits 1. Acquired pellicle 2. Dental plaque/biofilm 3. Dental calculus 4. Food debris 5. Materia Alba
Acquired pellicle • composed of - salivary glycoproteins (mucins) - No cells, no minerals, no bacteria • structure - surface layer & sub-surface layer - homogenous - very thin 1-10um • clinical appearance - translucent & colorless, invisible to naked eye
Formation of pellicle • Spontaneous • Bacteria not necessary(forms in germ free animals) • Forms from salivary glycoproteins by selective adsorption • Reforms very rapidly on the clean tooth surface within seconds • Takes 1 week to mature
Function & Clinical significance of pellicle Protective functions: • Reservoir of ions eg., calcium, phosphate and fluoride ions • Acts as a semi-permeable membrane. (imp in demineralisation- remineralisation, allows ion exchange) • Restricts diffusion of acids - protects enamel from minor acid attack • Lubricant - can protect tooth from wear • Antibacterial factors – IgA, Lysozyme
Function & Clinical significance of pellicle Damaging functions • Influence while bacteria colonise the tooth (plays a role in the formation of Dental Plaque) • Nutrient supply for some bacteria in dental plaque • Presence of pellicle alters surface energy of tooth (important by use of dental adhesive materials) • Difficult to remove with toothbrushing, professionalcleaning needed
Capnocytophaga species Porphyromonas Gingivalis Veillonella species Streptococci Fusobacterium species Motile gram-negative rods and spirochetes Other gram-positive rods Streptococci Streptococci Actinomyces species Prevotella intermedia Early colonizers Late colonizers
Dental plaque/Dental Biofilms Definition: It is a soft, non-mineralisedmicrobial deposit which forms on the hard tissue surfaces of the mouth (and dental prostheses), comprising living and dead bacteria and their products together with the host compounds mainly derived from saliva.
Dental plaque 1mg of plaque contains about 108 bacteria
Dental plaque is now commonly called a dental biofilm…. ..because…..
What are biofilms?? Biofilms are highly organized communities (cities) of microbes with their own: • nutrient delivery • waste disposal • communication • defences systems.
What are biofilms?? Microbial biofilms is composed of: • Bacteria • A matrix of: • Glycoproteins • Extracellular polysaccharides (glucans and fructans) • The entire structure is embedded in a sticky substrate produced by the bacteria. • The substrate holds the microbial city together & adheres it to the pellicle.
What are biofilms?? • The adherence through the matrix makes it impossible to rinse it away and have to be removed mechanically (scaling, toothbrushing etc.) • Differing environments exist within the microcolonies (pH, oxygen) • Microorganisms in biofilms can be resistant to antibiotics, antimicrobials (eg some mouth-rinses), and host defenses
What are biofilms?? • Colour • If thin – it is invisible • If thick – variable clinic appearance adults: white -yellowish children: white – can be coloured (brown, orange, green - dependson type of bacteria – chromogenic bacteria can cause plaque to be coloured) • Texture – sticky • Thickness – variable
What are biofilms?? • Distribution: Plaque is categorized as: • Supragingival • Fissure plaque- mainly in molar fissures. • Approximal plaque • Smooth surface • Subgingival