Download
1 / 43
430 likes | 927 Views
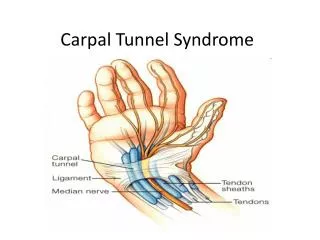
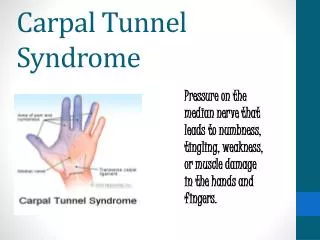
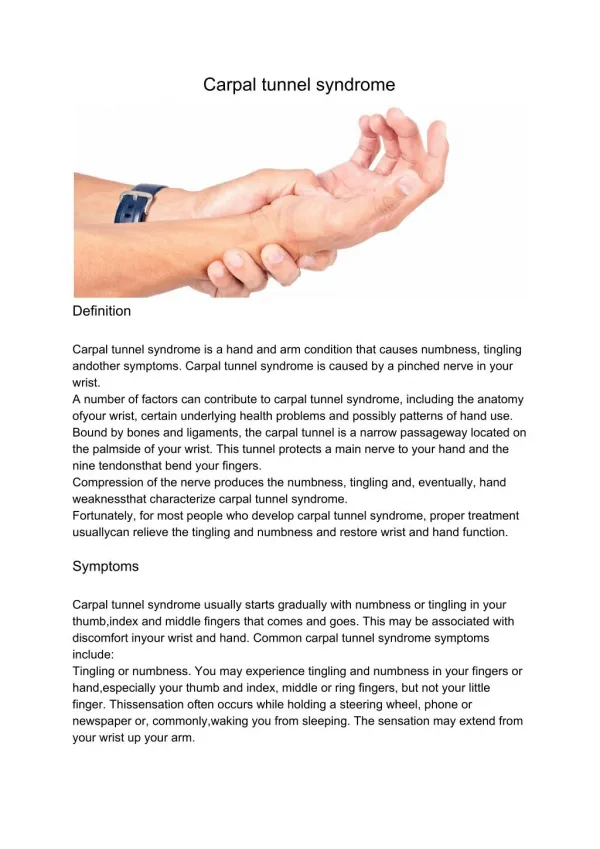
CARPAL TUNNEL SYNDROME. It is a compression of the median nerve (Figure 1) at the level of the carpal tunnel . Causes: 1- Trauma: Fracture and dislocation 2- Increase in volume of tunnel contents secondary to: a ) Tenosynovitis

E N D
It is a compression of the median nerve (Figure 1) at the level of the carpal tunnel. Causes: 1- Trauma: Fracture and dislocation 2- Increase in volume of tunnel contents secondary to: a) Tenosynovitis b)Thickening of the transverse carpal ligament 3- Tumour.
Pathology: 1. In acute compression a severe deforming force (traumatic dislocation of the carpal bones) cause mechanical deformation of the carpal tunnel and ischemic changes of the median nerve. 2. Chronic compressive compression: Stage I: Progressive obstruction of the venous return causing circulatory slowing in the epineural and intrafuniculartissues,which leads to impairs the nerve fibers nutrition. The hypoxic nerve become hyperexcitable and discharge spontaneously. Pain and parethesia result from the imbalance of fiber activity and fiber dissociation. Nocturnal paresthesia and pain are caused by impeded venous return from distal part of the thumb. At this stage, the structural changes may be corrected by treatment that eliminates or reduce pressure in the carpal tunnel.
Stage ll: The capillary circulation slows so severely, that anoxiadamages the endoneurim. Edema occurs as protein leaks into the surrounding tissue. Within the funiculi, endoneural tissue accumulates protein, which interferes with the nutrition and metabolism of the nerve fibers. Protein exudates promote the proliferation of fibroblasts and the formation of constrictive endoneurial connective tissue. Segmental demylination, axon thinning and destruction of axons are found in individual nerve fibers.
Stage III:Nerve fibers undergo Wallerian degeneration with loss of axons available for regeneration. The compressed nerve become a Fibrous cord. Patient Complaints: 1-Pain 2-Weakness 3-Occasional burning shoulder pain 4-Stage I chronic compression is indicated by nocturnal pain and diminished sensation in the distribution of the median nerve. 5-Stage II is indicated by burning pain and referred to the shoulder. 6-Stage III is indicated by pain subsidence or it become more severe. 7-Acute compression is indicated by numbness or severe pain.
Evaluation: • Diminished sensation in the thumb, index, long and radial aspect of Ring fingers. • Atrophy of thenar muscles • A positive tinel's sign (Figure 2) • Positive phalen's sign (Figure 2 • visual inspection of the hand for pseudo-motor changes in the skin • X- ray views of the carpal tunnel • EMG and nerve conduction • Hand grip dynamometer
Figure 2: Left, The examiner taps the hand from the fingertips proximally to the palm. The patient is asked to report any "electric shocks" or tingling when percussed. Right, The patient is asked to report any sensory changes in the median nerve innervated area after holding his wrists flexed for 1 minute.
Non operative management • Initial treatment by a physician may include local steroid injection, oral NSAI. • Splinting by the volar wrist cock up splint, the wrist in 10 to 20 degrees of extension . It is wearied continuously for 4 to 6 weeks, and decrease use of splint over the subsequent 4 weeks (Figure 3).
Instruction to avoid certain wrist and hand postures (Figure 4). These includes: • Gripping or pinching objects while flexing the wrist • Performing repetitive wrist flexion extension motion • Gripping a tool by ulnardeviating hand. Examples: • Computer keyboard typing • Driving long distances • Use of tools that produce vibrations in the hand, such as: hammers, saws, drills, and jack-hammers • Repetitive assembly line work • Folding materials such as laundry and paper products • Knitting and sewing 4. Control inflammation through ice packs, tendon gliding exercises (Figure5) performed 5 times each, 5 times daily, and elevated activities
Figure 3: The custom-design volar wrist—extension splint can be used during work activities. The patient is taught how to maintain flexor muscle relaxation while wearing the splint.
Figure 4: Flexing the wrist, prolonged reaching , and working with vibrating tools can result in compression of the median nerv. Gripping a tool by ulnar deviating the wrist can aggravate themedian nerve within the carpal tunnel.
Figure 5: Tendon gliding exercisesa straight palm...then a hooked fist.. ...now make a "straight' fist ...and a full fist
Post surgical management: Goals for the first 3 weeks postoperative: • Control edema • Maintenance of ROM • Restriction of adhesion formation • Protected use of the hand Methods: 1-Constant elevation of the involved hand , and retrograde massage. 2-Tendon gliding exercise: 10 repetitions, 3 times daily. 3-Shoulder exercises are performed 3 times daily in all directions. 4-After one week the volar cast is removed and another thermoplastic splint is fabricated to be worn during sleep and strenuous activities
Goals for those requiring further treatment 3 to 8 weeks: • Reducing edema • Modeling the scar • Reducing hypersensitivity • Increasing strength and functional use • Increasing ROM Methods: • Overhead bilateral fisting exercises 10 repetitions per hour and retrograde massage. • Elastomeris applied to the palmar scar to model it • Desensitization program • Isometric and Isotonic exercise for the wrist and hand by the 8th week (do not overexercise). • Nerve gliding exercises (Figure 6), tendon gliding exercises and passive stretch of the thumb (3 time per day for 10 repetitions each)
Figure 6: Nerve gliding exercises are initiated to facilitate mobilization of the median nerve 1. Wrist in neutral, fingers and thumb in flexion.2 Wrist in neutral, fingers and thumb extended.3. Thumb in neutral, Wrist and Fingers extended.
4. Wrist, fingers and thumb extended.5. Same as position 4. with forearm in supination, (palm up)6. Same as position 5. other hand gently stretching thumb.
At 8 to 12 weeks: • Work hard is initiated • Light house repair • House cleaning • Light work tasks Tolerance program: Work tolerance is evaluated as he performs repetitive exercises and job simulation. If swelling or symptoms occur the length of treatment is prolonged 4 additional weeks .
Patient with Ions histories of chronic progressive compression may need further treatment for pain control: • High voltage galvanic stimulation • TENS • Contrast bath: cool water for 30 sec and warm water for 30 sec for 15 to 3 0 min. • Massage • Splint use • Phonophoresis.
DE QUERVAINS DISEASE The thumb plays a main role in hand function. It is subjected to an "overuse" phenomenon which was first identified in the 1893 edition of gray's anatomy as Washerwomen's sprain. In 1895 this condition was further described by the Swiss surgeon Fritz de Quervain as a stenosing tenosynovitis in the first dorsal compartment which contains the abductor pollicis longus and extensor pollicis brevis tendons.
Anatomy: Six tunnels or compartments are formed beneath the extensor retinacululm. The abductor pollicis longus and the extensor pollicis brevis tendon share a common synovial sheath extending approximately l cm distal to the extensor retinaculum. These tendons pass through a shallow groove over the prominence of the radial styloid. Tenosynovitis results from friction between the tendon, the tendon sheath and the shearing of the tendons against the bony groove of the radius.
Causes: • In manual laborers who combine pinch with wrist motion and forearm rotation have persistent strain as these motions are performed rapidly and repetitively over the course of time. • Repetitive pressure, voluntary motion, over exertions, lifting objects, pulling objects or throwing objects all can produce tenosynovitis.
Pathology: • Movement of the tendons cause secretion of lubricating fluid, which may not increase in proportion to the amount of tendon use leading to tenosynovitis • There is congestion of the serum and fibrin within the wall of the sheath. Tenosynovitis occurs when serum is reabsorbed, thus contributing to adherence between the synovium and the tendon. • The tendon may become flattened and thinned and covered with granulation tissue which may cause formation of connecting fibrous band and produce thickening of the tendon . • As the fibrous sheath become further inflamed and edematous the tendons are constricted in this area. • As a sequel of these changes a loss of blood flow may result affecting the nutritional states of the area.
Symptoms: Discomfort over the radial aspect of the wrist, which may radiate proximally up to the forearm and distally into the thumb. This pain is aggravated by thumb and wrist motion especially active or resistive extension and abduction of the thumb. Evaluation: • On palpation the following was detected: • Localized tenderness approximately 1 cm proximal to the styloid process. • The area of the extensor sheath may appear and feel thickened. 2) Finkelestin test (Figure 2): This test produces localized pain over the abductor pollicislongus tendon in the first dorsal compartment. 3) To rule out the extensor pollicislongusinvolvement, positions the wrist in neutral and stabilizes the CMC and MP joints of thumb while testing resisted IP joints extension. Any discomfort reported by the patient should be noted.
4) Therapist's interview: a)The therapist must inquire about positions, tools and equipment that the patient may use to perform job. b)The patient's activity of daily living status must be obtained, c) Assess pain by: • 10 cm pain analogue scale • The area of pain • The time of day pain • The corresponding activity that may elicit pain • The duration of pain • The posture of the extremity that reproduce pain symptoms
5) Note the attitude of the thumb at rest and check for signs of edema on the radial aspect of the wrist, in the area of the first dorsal compartment, and throughout the thumb. 6) Edema assessment by volumetric readings or tape measurement taken at the level of the wrist or at the distal palmar creases. Jeweler's ring may be taken at the usual thumb landmarks. 7) Motion of the affected thumb and wrist may be normal or slightly limited. The ability to oppose the fingertips and the volar head of the 5th metacarpal or ulnar aspect of the distal palmar crease is also documented. Contracture of the first web space must be assessed. 8) Strength testing (Figure 3)
Treatment Conservative approach: If the patient has symptoms less than 6 month, a conservative approach may be initiated. A) Initial phase (1-4 weeks) 1. The patient may receive 2 to 4 steroid injections into the first dorsal compartment. 2. Rest for the tendons of the first and second dorsal compartment.
The rest is provided by: • A forearm bases splint (Figure 4) which may be referred to as long opponens or a long thumb spica splint. Its design immobilize the wrist and the CMC and MP joints of the thumb, the IP joint is left free. The wrist at 15 degrees extension, the CMC joint at 40 to 45 degrees of palmar abduction, the MP at 5 to 10 degrees flexion and the IP joint is free. The splint should be worn at all times with the exception of removal for hygiene and exercise. The splint may be removed 3 times daily for exercise.
3. Exercises: a. Active ROM exercise to prevent stiffness and possible adhesion between the tendons and the synovial sheath. b. Gentle passive and active wrist and thumb motions in all planes are encouraged. c. During the first week, a light program of exercise is performed. If the patient demonstrates the ability to withstand an increased number ofrepetitions in the day that follows, light prehension activities may be initiated:
The patient begin grasp and release of small light weight objects (foam pieces, cotton balls, spools, checkers) using various pattern of prehension. • Towel gathering and unfolding activities (Figure 5) which may later be dvanced to a more resistive paper crumpling activities. • Short exercise periods ranging from 10 to 20 min. Only as the patient demonstrates increased tolerance for activity should the program be expanded. • For the periods when the patient's splint is on, a proximal joint ROM is provided to enhance circulation, to minimize joint stiffness and protective posturing and to maintain functional motion of the affected extremity.
4. Monitor edema for the first day of treatment: • While wearing the splint, maintain the affected hand above the heart level as much as possible. • Overhead intermittent pumping of the fingers every hour. • Wear compressive stockinette encompassing all MP joints, the wrist and the forearm. 5. Technique used to assist with control of the inflammatory stage: A-Retrograde lotion massage 4 times per day B-Cryotherapyin the form of ice pack lasting from 10 to 15 min with a thin moist towel. Also ice massage, avoiding bony prominences, for a maximum duration of 5 min.
C-Contrast bathperfomed in elevation (increase metabolic and phagocitic acitivity). Squeezing sponge in the bath may be too resistive initially, so the patient is taught instead to gently move the thumb to the lateral aspect of the index while pumping the fingers in one bath. In the other bath,gentle wrist motion may be performed. D-Phonophoresis: Apply heat before phonophoresis to improve conduction through the skin (10% hydrocortisone, 10 to 12 daily sessions of 5 min.
Figure 4:The splint design for the patient with de quervain's disease immobilizes the entire or radial aspect of the wrist and includes the carpometacarpal and metacarpophalangeal joints of the thumb.
B) Second phase (4 to 12 weeks) If progress occurs in edema reduction, pain free motion, the patient advances to the second phase of treatment. 1-Splint.The patient is gradually weaned from his protective splint. The patient continues to wear the splint throughout the night and decrease weaning time during the day. During the day, it is best to incorporate a semiflexible external support (Figure 6) to limit extremes of motions. 2-Thumb protection technique: is used during this phase. It includes avoidance of prolonged pinch, forceful thumb flexion, repetitive thumb motions, and combined pinch or grip with repetitive wrist motion in any plane. 3-Activity of daily living are reviewed and the patient is taught alternative methods to approach a task and to incorporate adaptive equipment.
4-Exercise session: Elongate the light activity exercises as follow: a) Gentle isometric (Figure 7) strengthening may be initiated for 5 min,3timesper day. Various dowels may be pushed through putty while first stabilizingthe thumb on the proximal phalanx of the index finger, progressing to a position where the thumb encompasses the dowel, and pushing the dowel with the thumb. b) Isotonic exercises: (Figure 8) The forearm and wrist in a neutral position and holding a dowel or pencil as the fingers provide a graded resistance to the activity, then the thumb assist in returning the pencil back to the original position. Use of syringe, putty pinching, and link belt fabrication, all are use as a type of isotonic exercises. Lateral pinch must be accomplished before opposition.
c) Isometric wrist strengthening is performed. Grasp of 1 ounce to 3 pounds weight assists the patient in regaining muscle strength. d) Isotonic wrist strengthening using weights, tools, Baltimore therapeutic equipment (BTE). and work simulator. 5. For job: Lifting, carrying, reaching, grasping, tool, handling and pinching are initiated for short periods while using the affected wrist and thumb in midrange. Adaptation in work might include: • Returning to a shortened work day • Rotating workstations to ensure changes in hand positioning. • Allowing the patient to use a flexible support during work. • Permitting the patient to attend therapy once a week
Figure 6: A semi flexible support may be fabricated to limit extremes of motion
Figure 7: Isometric strengthening may be initiated by pushing a dowel through putty
Figure 8: Isotonic strengthening may be initiated by pushing the thumb down on a pencil while the fingers graded resistance then actively using the thumb extensors to help push the pencil backup to its original.
Post surgical approach: Indication for surgery: No relief of symptoms after a trial treatment of 3 to 6 weeks. The tendons are decompressed and adhesions are dissected. Physiotherapy program: Start physiotherapy after the third day, by assessing ROM, edema and pain • Apply thermoplastic splint (wrist neutral to slight extension and thumb neutral while the fingers free. (Figure 4) • Edema control (cold pack application, elevation, compressive stockinet, retrograde massage avoiding the wound area and intermittent compression pump.
3) Tendon gliding exercise of uninvolved digits 5 times per day. 4) Active motion for the wrist, CMC, MP and IP joints of the thumb. 5) Gentle passive ROM if stiffness is noted. 6) Biofeedback may be considered for some patient because thumb extensors appear more active than necessary even at rest. 7) If there is prolonged hypersensitivity in the area of surgical site exists desensitization program is used. Methods of counter irritation such as the use of heat, cold, and TENS may be tried. 8) After suture removed at the 8th-10thday, massage is recommended (pressure massage 5 sec per area) on the perimeter and later over the surgical site. Ultrasound may be applied over the scar to assist in the disruption of the "connective tissues polypeptide bonds. 9) The remainder of the patient's postsurgical program is the same as for conservative management.