Download
1 / 23
230 likes | 344 Views
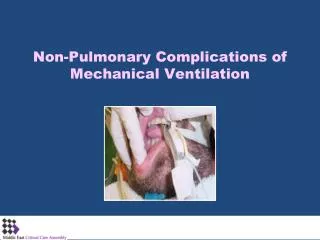
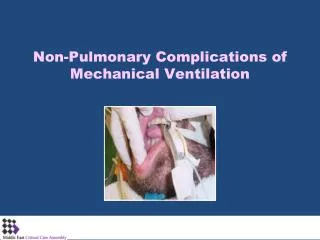
Complications: Revisions MISS 2010. Bruce M. Wolfe Professor of Surgery Oregon Health & Science University. Complications: Revisions. Provider error Large gastric pouch Incomplete gastric division Incorrect limbs. Complications: Revisions. Patient and/or provider factors Marginal ulcer

E N D
Complications: RevisionsMISS 2010 Bruce M. Wolfe Professor of Surgery Oregon Health & Science University
Complications: Revisions • Provider error • Large gastric pouch • Incomplete gastric division • Incorrect limbs
Complications: Revisions • Patient and/or provider factors • Marginal ulcer • Stricture • Intestinal obstruction
Complications: Revisions • Poor weight loss or regain • Anatomic factor • Gastric pouch size • Dilated gastrojejunostomy • Gastrogastric fistula • Patient factor • Operative anatomy as expected
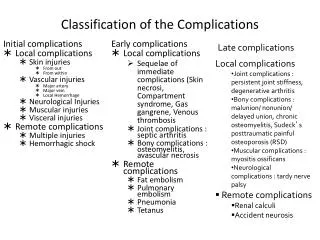
Marginal Ulcer • Evaluation • Endoscopy • UGI • Intraoperative endoscopy • Define pouch • Confirm resection • Test anastomosis • ± Vagotomy
Background • Revisional bariatric surgery • Indications: • Side effects or complications of prior bariatric surgery • Inadequate weight loss • Higher morbidity than with first time procedures
UWashington/ VMason NRI/UND OHSU/ Legacy Sacramento Bariatric GSPH Columbia/ Cornell UPMC NIDDK/ ORWH ECU Clinical Center Data Coordinating Center NIDDK / ORWH
Aim • To determine independent risk factors for adverse outcome in patients undergoing revisional bariatric surgery • To compare the outcome between first-time and revisional bariatric cases
LABS-1 Total 5069 patients/operations 30 Second stage procedures 6 Other secondary obesity procedures 5033 Primary, revisional or reversal operations 1230 Adjustable gastric banding 3803 stapled bariatric procedures 1 patient underwent 2 separate procedures: a revision followed by a reversal; The reversal was excluded from the analysis 3802 patients/operations 3577 primary procedures 225 revision/reversal procedures
Data definitions • Composite endpoint (CE) • Death • Deep venous thrombosis (DVT) or venothromboembolism (VTE) • Re-intervention with percutaneous, endoscopic or operative techniques • Failure to discharge within 30-days of surgery
Statistical Analysis • Characteristics across subgroups: • Categorical variables: • Pearson’s chi-square test • Continuous: • Kruskal-Wallis test • 30-day adverse outcomes: • Fisher’s exact test • Association between baseline patient characteristics and the odds of 30-day adverse outcome : • Multivariable generalized linear logistic regression models
Revisional vs. Primary Unadjusted Odds of CE is more than twice high for revisional surgeries compared to primary surgeries (OR = 2.4, 95% CI 1.6-3.6)
Revisional vs. Primary Adjusted for important comorbidities and other patient characteristics, odds of CE was more than twice as high for revisional surgeries compared to primary surgeries (OR = 2.3, 95% CI 1.5-3.8)
Conclusions • Revisional bariatric surgery can be performed without substantial mortality but with a greater incidence of adverse outcome compared to primary surgery
Acknowledgments This clinical study was a cooperative agreement funded by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Grant numbers: DCC -U01 DK066557; Columbia-Presbyterian - U01-DK66667; University of Washington - U01-DK66568 (in collaboration with GCRC, Grant M01RR-00037); Neuropsychiatric Research Institute - U01-DK66471; East Carolina University – U01-DK66526; University of Pittsburgh Medical Center – U01-DK66585; Oregon Health & Science University – U01-DK66555. The authors thank the LABS study participants for their contributions.