Download
1 / 29
290 likes | 421 Views
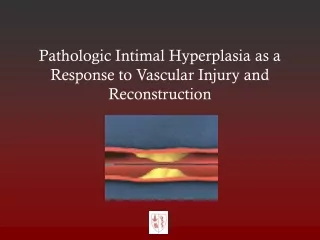
Immunophenotyping Intimal Arteritis. Anthony Chang, MD University of Chicago Medical Center. Immunophenotyping intimal arteritis.

E N D
Immunophenotyping Intimal Arteritis Anthony Chang, MD University of Chicago Medical Center
Immunophenotyping intimal arteritis • Is there a difference in the immunophenotype of lymphocytes in the setting of intimal arteritis associated with T cell-mediated rejection (TCMR) versus antibody-mediated rejection (AMR)?
Literature Review • Intimal arteritis immunophenotype studies • Tuazon TV et al. Am J Pathol 1987 • CD8, CD4 • Alpers C, et al. Mod Pathol 1990 • CD45, UCHL-1 (CD45RO or memory T cells) • L-26 (CD20+ B cells) • HAM-56 (macrophages, endothelium) • Leu-M1 (CD15 granulocytes), Factor VIII and Ulex uropaeus (endothelium), HHF-35 (smooth muscle actin), S100 (DCs, some macrophages) • 22 cases
Literature Review • Intimal arteritis immunophenotype studies • Matheson P, et al. Transplantation 2005 • UCHL-1 (CD45RO T cells) • CD68 (macrophages) • 8 of 24 bxs with type II or III rejection • CD68 > UCHL-1 • Kozakowski N, et al. NDT 2009 • CD68/CD3 ratio in 116 arteries from 34 patients • Did not correlate with C4d • Did not correlate with worse graft survival
Literature Review • Intimal arteritis immunophenotype studies • Sementilli A, et al. Tx Proceedings 2010 • CD68, CD4/CD8, CD20, S100 • IL-4, IL-10, interferon-gamma • 10 of 40 bxs with type II rejection • CD8 > CD68
Immunophenotyping intimal arteritis • Is immunophenotype of lymphocytes in the setting of intimal arteritis associated with T cell-mediated rejection (TCMR) different from the lymphocytes associated with antibody-mediated rejection (AMR)?
Our study • Intimal arteritis/endarteritis lesions • U of Chicago Med Ctr (n=20) • Cedar Sinai Med Ctr (n=12) • 15 – AMR only, 11 – TCMR+AMR, 6 – TCMR only • Immunohistochemistry • CD3, CD8, CD4, Foxp3 • CD20 • CD68 and CD163 • CD56
Tregs (CD4+/foxp3+) 1 of 13 cases
CD163 • Scavenger receptor • Limited to macrophage/monocyte lineage
CD68 / CD163 CD68 CD163
CD20+ B cells • 5 of 29 cases with any CD20+ B cells • 2 with isolated v lesions and C4d+ • 1 DSA+ class II, 1 DSA+ class I+II • 1 with isolated v lesion • C4d+ 5% of ptc, DSA/PRA-not tested • 1 with TCMR and AMR • C4d+ 5-10% of ptc, high PRA class I/II, DSA- • 1 isolated v lesion • C4d-, PRA/DSA- • 15 isolated v lesions with AMR only
CD56 (NCAM) • 9 CD56+ cases • No more than 4 CD56+ NK cell present • 2 cases with CD56 granular staining only; no CD56+ lymphocytes • Of 9 isolated v lesions • 7 with either CD56+ cell (n=5) or granular staining (n=2) • 7 of 10 CD56 staining with AMR alone • 0 of 2 CD56 staining in TCMR alone • 2 of 10 CD56 staining in TCMR+AMR
Summary • CD56 may be a useful marker to distinguish intimal arteritis associated with AMR from TCMR • Additional studies • CD20 – infrequent • CD3, CD8, CD68, CD163 – no significant difference
Acknowledgement • Collaborators • Mark Haas, Cedars Sinai Medical Center