Download
1 / 79
790 likes | 869 Views
THE GALLBLADDER. I. Introduction/General Information A. Location: 1. Epigastric region 2. Right hypochondriac region 3. On inferior surface of liver 4. Between quadrate and right lobes B. Pear-shaped, hollow structure.

E N D
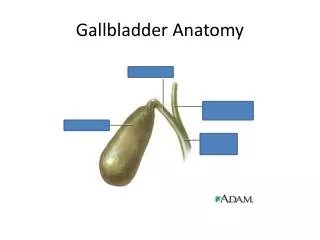
I. Introduction/General Information A. Location: 1. Epigastric region 2. Right hypochondriac region 3. On inferior surface of liver 4. Between quadrate and right lobes B. Pear-shaped, hollow structure
Introduction/General Information, con’t. C. Fundus slants inferiorly, to the right D. Attached to liver by loose (areolar) connective tissue E. Peritoneum covers free surfaces
Introduction, continued … F. Normal measurements: 7-10 cm long ~ 6 cm diameter 30 – 35 cc volume G. Body and neck directed toward porta hepatis
Introduction, continued … H. Neck is continuous with cystic duct I. Cystic duct: 1. joins common hepatic duct 2. superior and posterior to pylorus of stomach
Introduction, continued … J. Common Bile Duct 1. 10-15 cm long 2. Courses through lesser omentum 3. Deep to pyloric sphincter 4. Narrow tube, 1-2 mm diameter 5. Should be no more than 6 mm in diameter
CBD, continued … 6. May be 8-10 mm in post- cholecystectomy patients 7. Normally has smooth walls 8. Joins with pancreatic duct 9. convergence is seen a. anterior to portal vein b. posterior to head of pancreas
Introduction, continued … K. Combined duct empties into duodenum @ ampulla of Vater L. Sphincter of Oddi guards duct, regulates bile flow • Closed: bile goes into gallbladder • Open: bile goes into duodenum
II. Detailed Anatomy A. Fundus of GB: 1. may be palpated 2. in angle between lateral border of right rectus abdominis and costal margin 3. At level of elbow 4. Most anterior visceral structure
Detailed Anatomy, con’t. B. Body of Gallbladder 1. Visceral surface of liver 2. Deep to transverse colon or hepatic flexure of colon 3. Descending portion of duodenum is medial
Detailed anatomy, continued … G. Cystic Duct 1. 3-4 cm long 2. Extends from neck of gallbladder to common hepatic duct 3. Joins with common hepatic duct inferior to porta hepatis 4. Spiral valve may extend into neck of gallbladder
Biliary tract, continued … L. Blood supply to gallbladder: 1. Cystic artery a. arises (~ 60% of the time) from right hepatic artery b. passes posterior to hepatic duct, then divides
Gallbladder Diseases Cholelithiasis & Cholecystitis 1. Cholecystitis = inflammation of GB 2. Cholelithisis = Stone(s) in GB
Bile • Bile • Bile salts (primary: cholic, chenodeoxycholic acids; secondary: deoxycholic, lithocholic acids) • Phospholipids (90% lecithin) • Cholesterol • Cholesterol solubility depends on the relative concentration of cholesterol, bile salts, and phospholipid
Types of Gallstones • Mixed (80%) • Pure cholesterol (10%) • Pigmented (10%) • Black stones (contain Ca bilirubinate, cirrhosis and hemolysis) • Brown stones ( biliary tract infection)
Gallstone Pathogenesis • Pathogenesis of cholesterol gallstones involves: (1) cholesterol supersaturation in bile, (2) crystal nucleation, (3) gallbladder dysmotility, (4) gallbladder absorption • Black pigment stones: contain Ca++ salts, hemolytic conditions or cirrhosis, found in the gallbladder • Brown pigment stones: Asians, contain Ca++ palmitate, found in bile ducts, biliary dysmotility and bacterial infection
Gallstone Risk Factors • “Female, Fat, Forty, Fertile” • Oral contraceptives • Obesity • Rapid weight loss (gastric bypass pts) • Fatty diet • DM • Prolonged fasting • TPN • Ileal resection • Hemolytic states • Cirrhosis • Bile duct stasis (biliary stricture, congenital cysts, pancreatitis, sclerosing cholangitis) • IBD • Vagotomy • Hyperlipidemia
Cholecystitis (Acute & Chronic) ESSENTIAL FEATURES • Cholesterol stones form in 20% of women and 10% of men by age 60 • Cholesterol stone risk factors include: –Female gender –Age –Obesity –Estrogen exposure –Fatty diet –Rapid weight loss EPIDEMIOLOGY • Symptoms develop in about 3% of asymptomatic patients each year (20–30% over 20 years) • Acalculous cholecystitis affecting patients with acute, severe systemic illness
CLINICAL FINDINGS SYMPTOMS AND SIGNS • Biliary colic but becoming unremitting and steady in epigastrium or right upper quadrant • Fever • Nausea • Vomiting • Right upper quadrant pain to palpation with peritoneal signs • Murphy sign • Anorexia
LABORATORY FINDINGS • Leukocytosis IMAGING FINDINGS • Right upper quadrant US showing gallstones, gallbladder wall thickening (> 4 mm), or pericholecystic fluid (no stones if acalculous cholecystitis) • HIDA scan showing failure of filling of gallbladder (> 95% sensitive) • CT showing gallbladder wall thickening (> 4 mm), pericholecystic fluid (for patients with suspected acalculous cholecystitis) as sensitive as US
DIAGNOSTIC CONSIDERATIONS • Other causes of acute abdominal pain • Gallbladder: cholecystitis, choledocholithiasis, cholangitis • Duodenal ulcer • Hepatitis • Appendicitis (atypical presentation) • Pancreatitis RULE OUT • Choledocholithiasis • Pancreatitis
WORK-UP • History and physical exam • CBC • Amylase and lipase • Liver function tests • ALP, GGT • Right upper quadrant US • HIDA scan for difficult cases • CT if abdominal US not technically possible (patients with suspected acalculous cholecystitis, large wounds etc)
HIDA scan (Hepatobiliary Imino-Diacetic Acid scan) - radionuclide IV, extracted from blood, excreted into bile • Uptake by liver, GB, CBD, duodenum w/in 1hr = normal • Slow uptake = hepatic parenchymal disease • Filling of GB/CBD w/delayed or absent filling of intestine = obstruction of ampulla • Non-visualization of GB w/ filling of the CBD and duodenum = cystic duct obstruction and acute cholecystitis (95% sensitivity & specificity)
TREATMENT AND MANAGEMENT MEDICAL • All patients require IV fluids and antibiotics • Management then can include either early cholecystectomy (generally preferred) or cholecystectomy after about 6 weeks SURGERY • Laparoscopic cholecystectomy • Open cholecystectomy • Cholecystostomy tube (if cholecystectomy too hazardous) Indications • Suspected acute cholecystitis • Suspected acalculous cholecystitis • Failure to resolve cholecystitis on antibiotics
Complications • Bile duct injury or leak • Empyema –Suppurative cholecystitis occurs with frank pus in the gallbladder, high fever, chills and systemic toxicity –Percutaneous drainage or cholecystectomy is necessary • Pericholecystic abscess –Localized perforation at the gallbladder can result in a pericholecystic abscess –Treatment requires drainage with or without initial cholecystectomy • Free perforation –Rare but causes generalized peritonitis –This occurs when a gangrenous portion of the wall necroses prior to local adhesion formation –The diagnosis is rarely made before urgent laparotomy –Treatment is cholecystectomy • Cholecystoenteric fistula –Perforation at the gallbladder into an adjacent viscous generally resolves the acute episode –Symptomatic fistula and/or patients with continued gallstone symptoms should have cholecystectomy and closure at the fistula
Gallbladder Diseases, continued … Polyps of GB a. Intraluminal echogenic projections b. do not change position with patient c. Must be differentiated from septations, mucosal folds 1. septations extend across lumen 2. folds change configuration upon inspiration
Cholelithiasis ESSENTIAL FEATURES • Divided into symptomatic and asymptomatic • Caused by cholesterol (most common), black pigment, or brown pigment stones • Cholesterol stones form in 20% of women and 10% of men by age 60 • Cholesterol stone risk factors include: –Female gender –Age –Obesity –Estrogen exposure –Fatty diet –Rapid weight loss • Black pigment stone risk factors include: –Hemolytic disorders –Living in Asia • Brown pigment stone risk factors include: –Biliary stasis –Biliary infections EPIDEMIOLOGY • 20 million affected in United States • Symptoms develop in about 3% of asymptomatic patients each year (20–30% over 20 years) • Each year, complicated gallstone disease affects 3–5% of patients who are symptomatic
CLINICAL FINDINGS SYMPTOMS AND SIGNS • Asymptomatic • Biliary colic –Right upper quadrant or epigastric –Episodic, often after meals or at night, lasting as long as 2–4 hours • Nausea • Vomiting • Diarrhea • Mild right upper quadrant tenderness to palpation
LABORATORY FINDINGS • Normal liver function tests, normal amylase and lipase, normal WBC count IMAGING FINDINGS • Right upper quadrant US showing acoustically dense stones in gallbladder with acoustic shadowing without evidence of gallbladder wall thickening or pericholecystic fluid (> 90% sensitive for gallstones)
DIAGNOSTIC CONSIDERATIONS • Other causes of abdominal pain RULE OUT • Cholecystitis • Choledocholithiasis • Pancreatitis
WORK-UP • History and physical exam • CBC • Liver function tests • Amylase and lipase • Right upper quadrant US
TREATMENT AND MANAGEMENT SURGERY • Laparoscopic cholecystectomy • Open cholecystectomy Indications • Symptomatic cholelithiasis • Porcelain gallbladder (25% risk of carcinoma) Contraindications • First or third trimester of pregnancy (relative) • Previous upper abdominal surgeries (laparoscopic) Complications • Bile duct injury or leak
Cholelithiasis, Rare Complications ESSENTIAL FEATURES Gallstone Ileus • Small bowel obstruction secondary to 1 or more large gallstones entering via cholecystoduodenal fistula Mirizzi Syndrome • Biliary stricture secondary to direct compression by chronically impacted cystic duct gallstone or chronic inflammation secondary to chronically inflamed gallbladder EPIDEMIOLOGY • Both gallstone ileus and Mirizzi syndrome are rare complications mainly affecting patients older than 60 years
LABORATORY FINDINGS Gallstone Ileus • Hypokalemia • Prerenal azotemia • Hypernatremia • Leukocytosis Mirizzi Syndrome • Hyperbilirubinemia • Elevated alkaline phosphatase
IMAGING FINDINGS Gallstone Ileus • Abdominal x-ray –Air-fluid levels –Dilated loops of small bowel –Possible pneumobilia • US –Cholelithiasis and pneumobilia • Hypaque swallow –Fistula between duodenum and gallbladder Mirizzi Syndrome • US –Biliary dilatation (> 6 mm) –Cholelithiasis –Possible thickened wall of gallbladder • ERCP or percutaneous transhepatic cholangiogram (PTC) –Stricture of common bile duct
WORK-UP Gallstone Ileus • History and physical exam • CBC • Electrolytes • Blood urea nitrogen, creatinine • Plain abdominal x-ray • Right upper quadrant US • Small bowel contrast study if partial small bowel obstruction Mirizzi Syndrome • History and physical exam • CBC • Liver function tests • Right upper quadrant US
TREATMENT AND MANAGEMENT SURGERY Gallstone Ileus • Removal of retained small bowel gallstone(s) via enterostomy or partial resection if bowel damaged • Cholecystectomy and resection of fistula and duodenal closure at same operation or as staged procedure Mirizzi Syndrome • Cholecystectomy and resection and/or bypass of stricture via hepaticojejunostomy Contraindications • Clinical status of patient during laparotomy for gallstone ileus
Complications Gallstone Ileus • Missed enteral gallstone and recurrent obstruction • Duodenal leak • Bile duct injury or leak Mirizzi Syndrome • Anastomotic leak or stricture • Cholangitis
Choledocholithiasis & Gallstone Pancreatitis ESSENTIAL FEATURES • Cholesterol stone risk factors include: –Female gender –Age –Obesity –Estrogen exposure –Fatty diet –Rapid weight loss • Complicated gallstone disease affects < 0.5% annually of patients who are asymptomatic EPIDEMIOLOGY • Average age generally 10 years older than those affected by cholelithiasis (eg, 40–50 years of age)
CLINICAL FINDINGS SYMPTOMS AND SIGNS • Right upper quadrant pain • Painless jaundice • Both pain and jaundice • Fever • Asymptomatic • Nausea • Vomiting • Anorexia
LABORATORY FINDINGS • Conjugated hyperbilirubinemia (for choledocholithiasis) • Elevated alkaline phosphatase (for choledocholithiasis) • Leukocytosis (for pancreatitis or cholangitis) IMAGING FINDINGS • Right upper quadrant US showing presence of gallstones, dilated common bile duct (CBD) (> 6 mm) and CBD stone in only 20–30% of patients with choledocholithiasis • ERCP showing dilated CBD and presence of single or multiple CBD stones in patients with choledocholithiasis • ERCP showing impacted ampullary gallstone in < 10 % of patients with gallstone pancreatitis
DIAGNOSTIC CONSIDERATIONS • Presence of signs or symptoms suggestive of cholangitis RULE OUT • Biliary stricture
WORK-UP • History and physical exam • CBC • Liver function tests • Amylase and lipase • Right upper quadrant US • ERCP or laparoscopic cholangiogram
TREATMENT AND MANAGEMENT SURGERY • ERCP with sphincterotomy and stone extraction followed by laparoscopic cholecystectomy (preferred when cholangitis present or if pancreatitis does not resolve) • Laparoscopic cholecystectomy with CBD exploration • Laparoscopic cholecystectomy and cholangiogram followed by ERCP and stone extraction (preferred stone extraction technique is center specific for stones noted on screening cholangiogram following resolution of gallstone pancreatitis) • Percutaneous transhepatic cholangiography and stone extraction if ERCP unsuccessful and cholangitis present Indications • Choledocholithiasis noted to be symptomatic or asymptomatic • Gallstone pancreatitis MEDICATIONS • Antibiotics to cover GI flora for cases of cholangitis Complications • Pancreatitis (for ERCP) • Bile duct injury or leak Prognosis • Gallstone pancreatitis resolves in > 90% of cases Prevention • Treatment of symptomatic cholelithiasis
Choledochal Cyst ESSENTIAL FEATURES • Type I cysts (fusiform dilation of common bile duct [CBD]) account for 85–90% • Type II (true diverticula of CBD) 1–2% of cases • Type III (choledochocele–-dilation of distal/intramural portion of CBD) < 2% of cases • Type IV (multiple cysts involving intrahepatic and extrahepatic ducts) as high as 15% of cases in some series • Type V (cystic malformation of intrahepatic ducts) rare • 3–5% incidence of carcinoma EPIDEMIOLOGY • Onset of symptoms usually in infancy or childhood
CLINICAL FINDINGS SYMPTOMS AND SIGNS • Jaundice • Fever • Pain • Palpable right upper quadrant mass • Hepatomegaly • Bleeding varices • Asymptomatic
LABORATORY FINDINGS • Hyperbilirubinemia • Elevated alkaline phosphatase • Leukocytosis • Elevated amylase and lipase IMAGING FINDINGS • US showing characteristic cystic dilation of biliary tree corresponding to type as well as proximal dilation in presence of obstruction • ERCP or magnetic resonance cholangiopancreatography (MRCP) showing cystic dilation corresponding to type and proximal obstruction in presence of obstruction
WORK-UP • History and physical exam • Liver function tests • CBC • Amylase and lipase • Abdominal US • ERCP or MRCP (adults) • HIDA scan or MRCP (children)
TREATMENT AND MANAGEMENT SURGERY • Cyst excision and biliary reconstruction (types I–III) • Types IV and V individualized and may require partial hepatectomy if unilobar involvement TREATMENT MONITORING • Surveillance for carcinoma since patients still at increased risk for remainder of biliary tree Complications • Biliary stricture or leak • Cholangitis