Download
1 / 1
40 likes | 490 Views
Variable. Degree. ISS. LWD. P. N. 23. 26. Hand/wrist carpal wedging. Normal. 56.5. 30.8. 0.339. Mild. 13.0. 23.8. Variable. ISS. LWD. P. Moderate. 21.7. 34.6. N. %. N. %. Severe. 8.7. 11.5. 4 th Metacarpals short. 24. 20.8. 26. 15.4. 0.721. Radial lucency.

E N D
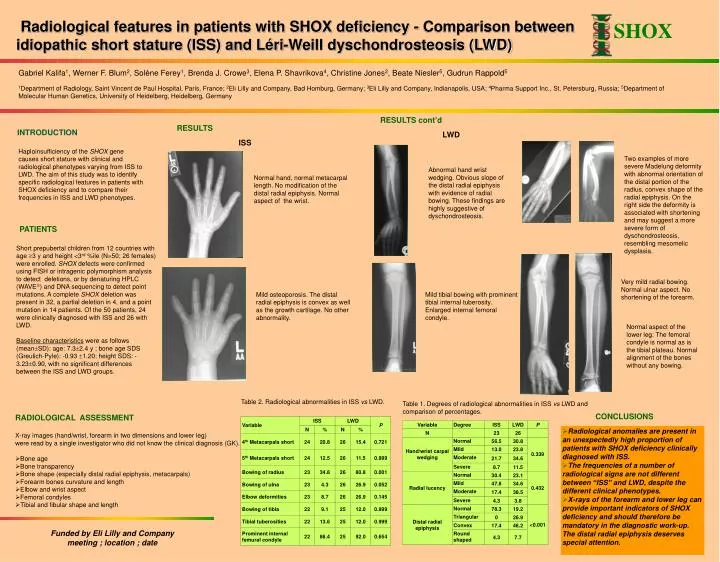
Variable Degree ISS LWD P N 23 26 Hand/wrist carpal wedging Normal 56.5 30.8 0.339 Mild 13.0 23.8 Variable ISS LWD P Moderate 21.7 34.6 N % N % Severe 8.7 11.5 4th Metacarpals short 24 20.8 26 15.4 0.721 Radial lucency Normal 30.4 23.1 0.432 Mild 47.8 34.6 5th Metacarpals short 24 12.5 26 11.5 0.999 Moderate 17.4 38.5 Bowing of radius 23 34.8 26 80.8 0.001 Severe 4.3 3.8 Distal radial epiphysis Normal 78.3 19.2 <0.001 Bowing of ulna 23 4.3 26 26.9 0.052 Triangular 0 26.9 Elbow deformities 23 8.7 26 26.9 0.145 Convex 17.4 46.2 Round shaped 4.3 7.7 Bowing of tibia 22 9.1 25 12.0 0.999 Tibial tuberosities 22 13.6 25 12.0 0.999 Prominent internal femural condyle 22 86.4 25 92.0 0.654 Radiological features in patients with SHOX deficiency - Comparison between idiopathic short stature (ISS) and Léri-Weill dyschondrosteosis (LWD) SHOX Gabriel Kalifa1, Werner F. Blum2, Solène Ferey1, Brenda J. Crowe3, Elena P. Shavrikova4, Christine Jones2, Beate Niesler5, Gudrun Rappold5 1Department of Radiology, Saint Vincent de Paul Hospital, Paris, France; 2Eli Lilly and Company, Bad Homburg, Germany; 3Eli Lilly and Company, Indianapolis, USA; 4Pharma Support Inc., St. Petersburg, Russia; 5Department of Molecular Human Genetics, University of Heidelberg, Heidelberg, Germany RESULTS cont’d RESULTS INTRODUCTION LWD ISS Haploinsufficiency of the SHOX gene causes short stature with clinical and radiological phenotypes varying from ISS to LWD. The aim of this study was to identify specific radiological features in patients with SHOX deficiency and to compare their frequencies in ISS and LWD phenotypes. Two examples of more severe Madelung deformity with abnormal orientation of the distal portion of the radius, convex shape of the radial epiphysis. On the right side the deformity is associated with shortening and may suggest a more severe form of dyschondrosteosis, resembling mesomelic dysplasia. Abnormal hand wrist wedging. Obvious slope of the distal radial epiphysis with evidence of radial bowing. These findings are highly suggestive of dyschondrosteosis. Normal hand, normal metacarpal length. No modification of the distal radial epiphysis. Normal aspect of the wrist. PATIENTS Short prepubertal children from 12 countries with age 3 y and height <3rd %ile (N=50; 26 females) were enrolled. SHOX defects were confirmed using FISH or intragenic polymorphism analysis to detect deletions, or by denaturing HPLC (WAVE) and DNA sequencing to detect point mutations. A complete SHOX deletion was present in 32, a partial deletion in 4, and a point mutation in 14 patients. Of the 50 patients, 24 were clinically diagnosed with ISS and 26 with LWD. Baseline characteristics were as follows (meanSD): age: 7.32.4 y ; bone age SDS (Greulich-Pyle): -0.93 1.20; height SDS: -3.230.90, with no significant differences between the ISS and LWD groups. Very mild radial bowing. Normal ulnar aspect. No shortening of the forearm. Mild osteoporosis. The distal radial epiphysis is convex as well as the growth cartilage. No other abnormality. Mild tibial bowing with prominent tibial internal tuberosity. Enlarged internal femoral condyle. Normal aspect of the lower leg: The femoral condyle is normal as is the tibial plateau. Normal alignment of the bones without any bowing. Table 2. Radiological abnormalities in ISS vs LWD. Table 1. Degrees of radiological abnormalities in ISS vs LWD and comparison of percentages. CONCLUSIONS RADIOLOGICAL ASSESSMENT • Radiological anomalies are present in an unexpectedly high proportion of patients with SHOX deficiency clinically diagnosed with ISS. • The frequencies of a number of radiological signs are not different between “ISS” and LWD, despite the different clinical phenotypes. • X-rays of the forearm and lower leg can provide important indicators of SHOX deficiency and should therefore be mandatory in the diagnostic work-up. The distal radial epiphysis deserves special attention. • X-ray images (hand/wrist, forearm in two dimensions and lower leg) • were read by a single investigator who did not know the clinical diagnosis (GK). • Bone age • Bone transparency • Bone shape (especially distal radial epiphysis, metacarpals) • Forearm bones curvature and length • Elbow and wrist aspect • Femoral condyles • Tibial and fibular shape and length Funded by Eli Lilly and Company meeting ; location ; date