Download
1 / 33
340 likes | 455 Views
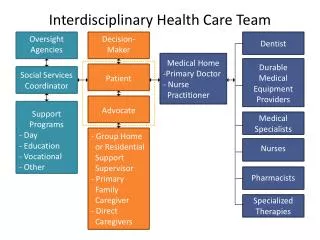
Community Health Team Care Management Process PinnacleHealth Systems. Don DeArmitt, M.D. Becky E. Zook RN, BSN, MS, CCP. Physician Champion Nurse Care Manager Chronic Care Initiative Nurse Medical Social Worker Behavioral Health Counselor Information Technologies Specialist.

E N D
Community Health TeamCare Management ProcessPinnacleHealth Systems Don DeArmitt, M.D. Becky E. Zook RN, BSN, MS, CCP
Physician Champion Nurse Care Manager Chronic Care Initiative Nurse Medical Social Worker Behavioral Health Counselor Information Technologies Specialist Community Health Team Members
Patient identification Manually- encounter with office staff Provider MA CHT member Self Automatically- high risk stratification report Quarterly on DM, HTN, CHF, CVD, COPD, Depression, Frail Elderly Daily- transitional care report Referral Process
Identify Patients with DM in Panel Determine Priority Patient Need Determine Delivery Mechanism Pt F/U with Provider Q6 months Low Risk 0-2 BP<130/80 A1c<6.5 LDL<100 Labs q6 months Phone F/U • Care Management • Monitoring (BG, BP, BMI, SM goals, etc) • Titration of meds • Home visit &/or phone F/U Q3 months Labs q3 months Medium Risk 3-5 p BP>130/80<140/90 A1c 6.6-8.0 LDL>100<130 BMI 30-35 • Medication • Monitoring • Titration up • Advanced Self Care • DM Education • SM Support • Monitoring • Functional Ability • Transition Care Class with ADE High Risk >5 BP>140/90 A1c>8.0 LDL>130 BMI >35 Seen in ER/ Hospital Social Worker prn • Social Issues • Transportation • $$ for Meds • Abuse • Insurance, etc Behavioral Health prn
Refer to Care Manager *Having two or more of the concomitant factors (tobacco use, LDL>130 or HDL<40) moves patient up in risk stratification CHF Stage A: Asymptomatic Stage B: Structural heart disease w/o symptoms Stage C: Structural heart disease with prior/ current symptoms Mild activity intolerance, fatigue Palpitations Dyspnea/angina with activity Comfort at rest Stage D: Refractory CHF requiring specialized interventions Severe activity intolerance, fatigue Dyspnea Angina Fatigue Palpitations at rest Identifying and Managing High Risk Patients HTN Low Risk* Pre-HTN Systolic <120-139 Diastolic 80-89 Moderate Risk* Stage 1 Systolic 149-159 Diastolic 90-99 High Risk* Stage 2 BP> 160/90
Refer to Care Manager • COPD • High Risk patients will have additional diagnosis and: • OV for acute bronchitis • OV for acute sinusitis • >4 OV in 1 year for COPD • ER or hospitalization for COPD in last 1 year • 2 or more other chronic diagnosis • Frail Elderly • High Risk patients will have metrics and / or diagnosis of: • Age > 65 years • BMI < 15 • Dementia or dementia related disease • Personal history of falls • Acute Care • High Risk patients include: • In-patient Facility • Home Health Care • Transitional Care • Diagnosis of Sepsis • Depression, Mental Health • High Risk patients will have additional diagnosis of: • Substance Abuse • Drug and/or Alcohol abuse • Tobacco use • MDI 10 score of severe or major depression • 2 or more other chronic diagnosis • CVD • High Risk patients will have additional diagnosis of: • DVT • PE • CVA • CAD or MI or PVD • Stage 1 or 2 Hypertension • 2 or more other chronic diagnosis
Triage and Assignment Per task status- STAT or Routine Manually by CM- based upon risk stratifications and qualifying diagnosis, transitional and STAT referrals priority Initial outreach 1-2 days for STAT referrals 10 days for routine referrals 1-2 days from notification of discharge of transitional referrals Referral Process
Successful contact Documented in the telephone template section of the EMR, task sent back to provider with documentation attached Unsuccessful contact 3 Attempts documented in the EMR CHT Unable to Contact letter Close if no response in 10 days to letter Task provider Referral Process
Patient identified as appropriate for contact from CM Introduce CHT, scope and practice, role of CM and self management skills Discuss trigger diagnosis Assess prior knowledge of diagnosis Assess use of hospital or ED in last 4 weeks Initial Patient Screening
Patient identified as appropriate for contact from CM Assess PHQ2 from G.O. intake assessment Identify needed behavior / lifestyle changes and blockers to change Identification of care driver- PCP vs specialist Set initial goals, time to next contact, plan for intake assessment Initial Patient Screening
Initial assessment completed Pt in agreement with services from CHT Documented in the EMR under the appropriate disease management template for guided assessments Intake Assessment
Telephone Office visits with CM Home visits Review of previous encounter for status of POC Cumulative review of goals and update of goals Establish next expected contact Follow-up Encounters
Review of self management progress Self management support and teaching Identify any new care gaps, needed coordination or safety issues Medication or treatment updates Follow-up Encounters
Since April 2010 inception- served nearly 700 patients in 2 Family Care practices 48% increase in patients with an A1C of less than 7.0 Since June 2010, 12% decrease in total number of patients utilizing hospital based services Addition of Behavioral Health Services CHT Outcomes