Download
1 / 34
360 likes | 528 Views
HIV/AIDS 101. Definitions, Epidemiology, & Information. Presenters. Scott Mattson, M.A. (Applied Social Psychology) Health Promotion & Community Education Coordinator AIDS Committee of Windsor Instructor Departments of Psychology, Sociology & Anthropology University of Windsor.

E N D
HIV/AIDS 101 Definitions, Epidemiology, & Information
Presenters • Scott Mattson, M.A. (Applied Social Psychology) • Health Promotion & Community Education Coordinator • AIDS Committee of Windsor • Instructor • Departments of Psychology, Sociology & Anthropology • University of Windsor
Please Take Out a Sheet of Paper: • Do NOT put your name on it • In order to tailor our presentations to the community: • What questions do you have about HIV/AIDS? (Label each with a “Q”) • What misconceptions do others have about HIV/AIDS? (Label each with an “M”) • Turn in at the end of talk
HIV HIV stands for: Human Immunodeficiency Virus. Like all viruses, HIV cannot grow or reproduce on its own. In order to make new copies of itself it must infect the cells of a living organism.
HumanImmuno Deficiency Virus • HIV only infects Humans • You must be Human to get or to give HIV • Any Human can get it; HIV Does Not Discriminate.It does not just infect those from ‘risk groups’ (ie: gay men, injection drug users, etc…)
HumanImmuno Deficiency Virus • Immuno refers to our immune system ~ the system that fights germs, infections, etc… and works to keep us healthy. The immune system is made up of many parts, including the white blood cells, which are the cells that HIV attaches itself to and uses to replicate itself. • Deficiency simply means that something is lacking or not working properly. As the virus replicates itself, white blood cells are destroyed, making it harder for a person living with HIV to fight off illness and other infections.
Human Immuno Deficiency Virus • Any group of microscopic agents capable of infecting animals or plants. • Viruses require a host cell (like a parasite does) in order to survive and reproduce. • In the case of HIV, since human blood cells cannot live outside the body for very long, neither can HIV. • A virus cannot be cured, however they are often very fragile. In the case of HIV, there are four things that can kill the virus ~ air, heat, bleach and acid. Unfortunately, due to their own harmful side effects, none of these things can be used to kill HIV inside the body.
AIDS AIDS stands for: Acquired Immuno Deficiency Syndrome An AIDS diagnosis is given when an HIV+ person experiences one or more opportunistic infections. This indicates that the infected person’s immune system has become weak enough for them to become susceptible to serious illness. Other things used to measure the strength of an HIV+ person’s immune system are viral load and CD4 counts.
AcquiredImmuno Deficiency Syndrome Acquiredmeaning to ‘get’ something. AIDS is not an illness that is inherited genetically.
AcquiredImmunoDeficiencySyndrome Immuno Deficiency meaning the immune system is not working as well as it should.
AcquiredImmuno Deficiency Syndrome Syndrome: A syndrome is a collection of symptoms or illnesses that describe a particular condition. For example: • If the syndrome is a cold, then the symptoms might include runny nose, cough, congestion, sneezing, etc… A person with only one of these symptoms does not necessarily have a cold nor must a person with a cold have all these symptoms. • In the case of HIV, these illnesses are called opportunistic infections. Opportunistic Infections take advantage of the body’s weakened immune system, often leading to very serious health problems.
HIV/AIDS HIV/AIDS are not interchangeable terms. HIV + 0I_ AIDS actual physical thing that can get inside the body Opportunistic Infections (ie: pneumonia, tuberculosis, etc...) Immune system is weakened enough to be vulnerable to serious illness or infections.
Disease Progression AIDS AIDS: HIV plus one or more Opportunistic Infections HIV + Infected with one of the Opportunistic Infections Asymptomatic Period: HIV+ with no symptoms Symptomatic Period: HIV+ with symptoms (ie: cold & flu symptoms, night sweats, wasting, etc…) HIV Test~ nominal or non-nominal blood test. Window Period~It may take up to 3-6 months for the body to produce enough antibodies to show up on a test. A person is infectious immediately upon becoming infected. Seroconversion (point of infection)
Transmission Equation 3 1 + 1 + 1 = ____ Representative of the possibility of HIV Infection
Transmission Equation 1 + 1 + 1 =3 1 HIV+ Body Fluid Blood Semen Vaginal Fluids Breast Milk
Transmission Equation 1 + 1 + 1 =3 1 Direct access to the bloodstream Intravenous Needles Cuts Tears Open Sores
Transmission Equation 1 + 1 + 1 =3 1 Risk Activities Unsafe body art practices Sharing needles Unprotected SEX Mother to Child
Transmission Equation HIV + Body Fluid (blood, semen & pre-ejaculate, vaginal fluids, breast milk) + Direct Access to the Bloodstream (cuts, tears, fissures, IV needles, receptor cells) + Risk Activity (unprotected sex, sharing IV needles, unsafe body art, mom to child) = possibility of HIV INFECTION
Determinants of Health • Determinants of health are factors & conditions that have an influence on the health of the individuals and communities. • Determinants do not act in isolation from each other. • The complex interaction of these determinants has an impact on the health of individuals and communities.
Determinants of Health The Public Health Agency of Canada, under its Population Health Framework, recognizes the following determinants of health: • Income & Social Status • Social Support Networks • Education • Employment & Working Conditions • Social Environments • Physical Environments • Personal Health Practices & Coping Skills • Biology & Genetic Endowment • Health Child Development • Health Services • Gender • Culture
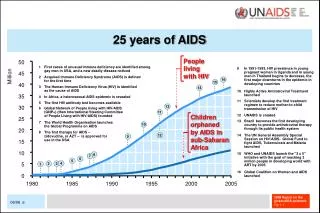
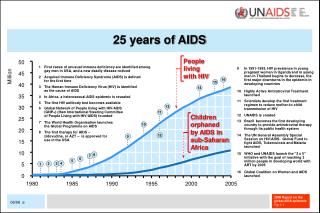
Adults & Children Living with HIV, 2006 (Estimated) Total: 39.5 (34.1–47.1) million UNAIDS, 2006. Available at: http://www.unaids.org
HIV/AIDS Canada • A total of 61,423 diagnoses of HIV infection have been reported to the Public Health Agency of Canada (PHAC) from November 1985, (when reporting began) up to June 30, 2006. • 20,493 diagnoses of AIDS from 1979 to June 2006. • For the first six months of 2006, a total of 1,232 diagnoses of HIV were reported, compared to 1,234 HIV diagnoses in the first half of 2005. • For the first half of 2006, 74.3% were male, 25.7% were female. • 47% were among men who have sex with men, 10.3% among injecting drug users, 33.5% among heterosexual contact exposure category
Positive HIV Test Reports in Canada:1995 - 2006 [JUN] Estimated
Report on HIV/AIDS in Ontario 2004 (February, 2006) • 25,251 Person living with HIV • 14,927 MSM • 3,356 From endemic regions • 3,367 heterosexual transmission • 2004 HIV Diagnoses • 1,690 in 2004 • + MSM, endemic, & heterosexuals • 28% Women (from 1.8% in 1985) • The most dramatic increase was in “low-risk heterosexuals”: +114% from 2000 to 2004
Biopsychosocial Impacts • HIV infection and AIDS affect all aspects of a person’s life. Those with HIV/AIDS must adapt to a chronic, life-threatening illness &corresponding physical, psychological, & social challenges. • Organic impairment to memory & thinking & side effects of anti-HIV drugs. • Common reactions to adverse life events & stigmatization: • Acute emotional distress, stress, anger, grief, helplessness, depression, anxiety, & cognitive disorders.
Testing in Windsor • Anonymous • HIV Care Program: 519-254-6115 • Anonymous (on request) or Confidential Testing for HIV & STIs • Windsor Essex County Health Unit: 519-258-2146 • Confidential • Chatham-Kent Public Health Services: 519-352-7270 • Only 66% (47%) of people who are infected know their diagnosis.
Confidential Information, Support, & Education • AIDS Committee of Windsor • 519-973-0222 • AIDS Support Chatham-Kent • 519-352-2121 • www.aidswindsor.org
HIV Care & Treatment • Anti- retroviral Treatment • Has increased the life span of PHA since introduction of HAART (Highly active antiretroviral) • Based on a combination of medications from various groups
FDA-Approved Drugs for HIV Therapy PIs NRTIs Amprenavir (APV) discontinued 2004 Atazanavir (ATV) Darunavir (DRV) Fosamprenavir (FPV) Indinavir (IDV) Lopinavir/ritonavir (LPV/RTV) Nelfinavir (NFV) Ritonavir (RTV) Saquinavir (SQV hgc) Tipranavir (TPV) Abacavir (ABC) Didanosine (ddI) Emtricitabine (FTC) Lamivudine (3TC) Stavudine (d4T) Tenofovir (TDF) Zalcitabine (ddC) withdrawn 2005 Zidovudine (ZDV) 3TC/ABC 3TC/ABC/ZDV 3TC/ZDV FTC/TDF Fusion Inhibitors (FIs) NNRTIs Enfuvirtide (ENF) Delavirdine (DLV) Efavirenz (EFV) Nevirapine (NVP) Multiple Class EFV/FTC/TDF
Approval of Antiretrovirals: 1987-2006 ATV FPV ENF FTC 25 DRV TPV 20 LPV/RTV TDF APV EFV ABC 15 NFV DLV Drugs RTV IDV NVP 10 SQV 3TC d4T 5 ddC ddI ZDV 0 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Year Figure does not include fixed-dose combinations.
Treatment & Prevention of OIs • Side Effects, Opportunistic Infections & Co-infections • Anemia • Diarrhea • Depression • TB • Dementia • Mycobacterium Avium Complex • Others (Diabetes, arthritis, etc.) • Psychosocial support provides coping skills that can bolster adherence • Nutritional support: also a prerequsisite for effective ART
Palliative Care • Strategies for end of life care: • Community home based care most cost-effective • Pain management: • Inexpensive options available, but significant barriers to access
Questions/Comments Thank you! (Please fold and turn in your sheet of questions/misconceptions)