Download
1 / 10

E N D
RHABDOMYOLYSIS What you need to know
“Rhabdomyolysis is a common disorder which may result from a large variety of diseases, trauma, or toxic insults to skeletal muscle. It may be defined as a clinical and biochemical syndrome resulting from an injury which damages the integrity of the sarcolemma of skeletal muscle, leading to the release of potentially toxic muscle cell components into the circulation…This may result in potential life-threatening complications including myoglobinuric acute renal failure, hyperkalaemia and cardiac arrest, disseminated intravascular coagulation, and more locally, compartment syndrome.” -http://members.tripod.com/~baggas/rhabdo.html
“We can dispose with much medical detail with a quick and easy description of rhabdomyolysis as a potentially lethal systemic meltdown initiated by the kidneys in response to the presence of shed muscle-fiber debris and exhaust in the bloodstream.” • Crossfit Journal 2005, Issue 38
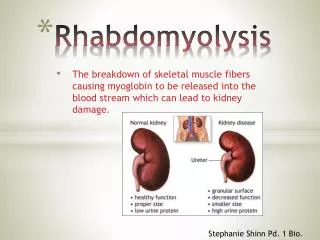
What Happens • Muscle cells are damaged • Releases muscle fiber content into the bloodstream • Potassium and myoglobin is released into bloodstream, calcium and sodium build up in the muscle cells • Myoglobin breaks down into ferrihemate in the kidneys • Kidney damage occurs, can cause acute renal failure (and death) • Potassium can cause alterations in heart function • High enough levels can cause arrythmia and heart failure (and death)
History • Five cases recorded with this type of workout • All athletes were previously involved in low-intensity, low power output workouts • All athletes were fit (ex: SWAT member, Special Forces member) • All athletes made a complete recovery • All continue to do this kind of workout (without another occurrence of rhabdo).
Drug Reactions • Toxic-mediated rhabdomyolysis may result from prescription and nonprescription medications, including the following: • Mevacore (lovastatin) • Antihistamines • Salicylates • Caffeine • Fibric acid derivatives (eg, bezafibrate, clofibrate, fenofibrate, gemfibrozil) • Neuroleptics • Anesthetic and paralytic agents (the malignant hyperthermia syndrome) • Amphotericin B • Quinine • Corticosteroids • Atorvastatin • Fluvastatin • Lovastatin • Pitavastatin (marketed in Japan, South Korea, India) • Pravastatin • Rosuvastatin • Simvastatin • Cerivastatin (recalled from US market) • Theophylline • Cyclic antidepressants • Selective serotonin reuptake inhibitors (the serotonin syndrome) • Aminocaproic acid • Phenylpropanolamine (recalled from US market) • Propofol (Continuous infusion has caused rhabdomyolysis in children.)
Substance Abuse • Toxin-mediated rhabdomyolysis may result from substance abuse, including abuse of the following: • Ethanol • Methanol • Ethylene glycol • Isopropanol • Heroin • Methadone • Barbiturates • Cocaine • Amphetamine • Phencyclidine • 3,4-methylenedioxymethamphetamine (MDMA, ecstasy) • Lysergic acid diethylamide (LSD)
Symptoms • Brown Urine • NOT yellow, go IMMEDIATELY to the hospital! • Muscle weakness • Extreme soreness that lasts more than two/three days
Prevention • Hydrate with water beforehand • At least four hours prior start drinking water • Stop all caffeine intake • Hydrate during and after the exercise • Monitor body signs throughout workout • Don’t work out or compete if you have a cold/flu • Rhabdo is EASY to prevent
Bibliography • Crossfit Journal 2005, Issue 38 • http://www.crossfit.com/cf-journal/rhabdo.pdf • Rhabdomyolysis • http://members.tripod.com/~baggas/rhabdo.html • eMedicine – Rhabdomyolysis • http://www.emedicine.com/emerg/topic508.htm