Download
1 / 73
870 likes | 2.37k Views
CRUSH INJURY AND RHABDOMYOLYSIS. Trauma and Critical Care Symposium Penrose-St. Francis Trauma Center Colorado Springs – May 2, 2013 Darren Malinoski, MD Associate Professor of Surgery Oregon Health & Science University. ROADMAP. General definitions History

E N D
CRUSH INJURY AND RHABDOMYOLYSIS Trauma and Critical Care Symposium Penrose-St. Francis Trauma Center Colorado Springs – May 2, 2013 Darren Malinoski, MD Associate Professor of Surgery Oregon Health & Science University
ROADMAP • General definitions • History • Pathophysiology of muscle injury • Pathophysiology of renal injury • Diagnosis • Treatment strategies • Thresholds for treatment • Natural disasters • Research at LAC/USC and OHSU
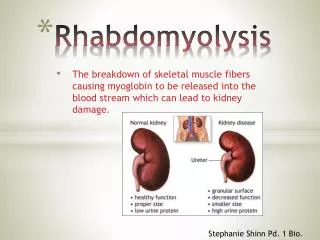
RHABDOMYOLYSIS • (Rhabdo): striped muscle dissolution. • Etiologies • Release of cellular contents into the circulation • How to measure/quantify • Treatment?
MYOGLOBIN • An oxygen-binding protein found within skeletal muscle that contains a single heme prosthetic group with an iron atom at the center that serves as the oxygen-binding site. Higher affinity for oxygen than hemoglobin which facilitates delivery to muscle.
CREATINE KINASE • CK: intramuscular enzyme that catalyzes the formation of ATP: ADP + creatine phosphate ATP + creatine • Several isoenzymes: CK-MM (striated muscle), CK-MB (cardiac), CK-BB (brain) • Normal plasma range 45-397 IU/L; plasma level of CK is proportional to degree of rhabdo CK
COMPARTMENT SYNDROME • Refers to the local manifestations of neuromuscular ischemia because of increased pressure within the osteofascial compartments. • Signs and symptoms • Diagnosis • Fluid sequestration
CRUSH SYNDROME • The systemic manifestations of muscle injury after direct trauma or ischemia-reperfusion injury. Commonly found in victims of earthquakes who have been caught under the rubble of collapsed buildings. • SIGNS AND SYMPTOMS: • Tense, edematous, painful muscles • Dark tea-colored urine • Shock • Acidosis • Acute renal failure
RENAL IMPACT • Acute Renal Failure (ARF): a decline in renal function severe enough to require some form of renal replacement therapy. • Many definitions • Mortality ranges from 5-50% when renal failure follows crush injury
HISTORY OF RHABDOMYOLYSIS • 1880’s: first reported in the German Literature • 1911: Meyer-Betz described a clinical syndrome consisting of dark brown urine, muscle pain, and weakness • 1941: Bywaters and Beall report 4 cases of crush syndrome during the bombing of London during WWII. They recognized the association between swollen extremities, hypovolemia, vaso-constriction, and eventual oliguria / renal failure.
CAUSES OF RHABDOMYOLYSIS • Alcohol intoxication, immobility, compression • Positioning during surgery • Seizure disorders • Medications: steroids, paralytics • Toxins: alcohol, cocaine, insect bites, reptiles • Costa Rican jumping viper venom • Genetic Disorders • Infection: bacterial and viral • Trauma: Crush injury / Vascular Occlusion
PATHOPHYSIOLOGY OF MUSCLE INJURY • Immediate cell disruption • Direct pressure on muscles • Stretch-activated channels opened – Ca++ influx • Ischemia/Anaerobic metabolism • Loss of cellular membrane integrity • Vascular compromise • Prolonged compression vs. vascular injury • Histologic changes at 2 hours • Necrosis at 6-8 hours
ISCHEMIA-REPERFUSION INJURY • Occurs when patients are extricated from collapsed buildings or when vascular flow is re-established: • Swelling of affected extremities / Compartment Syndrome • Hypovolemia / Shock • Free Radical formation • Lipid Peroxidation cell lysis • Toxin release: lactic acidosis, aciduria, myoglobinemia, CK, and thromboplastin (can DIC) • Electrolyte abnormalities: K, Phos, Ca
PATHOPHYSIOLOGY OF RENAL INJURY • Hypovolemia and Shock • Myoglobinuria: when plasma concentration exceeds 0.5-1.5 mg/dL, myoglobin filtered into urine. • Cast formation/tubular obstruction * • Free radical formation and lipid peroxidation * • Vaso-constrictor formation: PAF, endothelins *intensified by acidic urine
DIAGNOSIS • History • PEX • Labs: • Serum: CK, myoglobin • Urine: inspection, dipstick, myoglobin • Is general screening necessary?
TREATMENT • Prevention of Muscle Injury • Fasciotomy • Amputation • Prevention of Renal Injury • Dialysis
PREVENTION OF MUSCLE INJURY • Prompt restoration of blood flow • Delivery of intravenous fluid is the FIRST priority • Extricate victims from rubble NEXT • Reduce fractures and splint extremities • Repair vascular injuries
TREATMENT OF MUSCLE INJURY • Fasciotomy • Controversies: indications and timing • compartment pressure >30-50mmHg • DP <30 mmHg (diastolic minus compartment) • Amputation • if limb salvage is not possible • if the patient will die from intractable hyperkalemia, acidosis, or infection
White, et al. Elevated Intramuscular Compartment Pressures Do Not Influence Outcome after Tibial Fracture. JOT, 2003. • Hypothesis: Absolute intramuscular pressure measurements are non-specific and lead to unnecessary fasciotomies • Prospective analysis of 210 patients with tibial fractures • Continuous compartment pressure (CP) • Fasciotomy for DP >30 mmHg or clinical Dx • 109 pts either had Dx of compartment syndrome or elevated compartment pressures for less than 6 hrs. • 101 patients remained with CP > 30 mmHg
White, et al. Elevated Intramuscular Compartment Pressures Do Not Influence Outcome after Tibial Fracture. JOT, 2003. • 101 pts with elevated CP and normal DP • 41 patients: CP > 30 mmHg (30 to >70) • 60 pts: CP < 30 mmHg • None developed compartment syndrome • None required fasciotomy • No significant difference in outcome: • Sensory function, Muscle power, Peak torque, Functional indices of recovery
TO CUT or NOT TO CUT… • Irreversible muscle damage after 6-8 hours • Sheridan, et al. J Bone Joint Surg Am 1976 • Only 8% of pts with fasciotomy after 12 hours had restoration of normal function • 46% infection, 21% amputation • Bradley. Surg Gynecol Obstet. 1973 • Meta-analysis: 80% of pts with paralysis had unsatisfactory outcomes
TO CUT or NOT TO CUT… • Matsuoka, et al. J Trauma. 2002 • Increased disability in pts who underwent fasciotomy >12 hours after injury (47% vs 16%) • Seddon. J Bone Joint Surg Br. 1956 • Spontaneous recovery of muscle function up to 3 months after injury • Recommends delayed fasciotomy and release of ischemic contractures to maximize outcome • Better and Finkelstein condemn delayed fasciotomy due to risk of overwhelming infection
FASCIOTOMY • Two incisions • Lateral incision: • Anterior compartment • Lateral / Peroneal compartment • Medial incision: • Posterior compartments • One incision • Lateral: all four compartments
Split Thickness Skin Graft to close fasciotomy wound after several weeks.
PREVENTION OF RENAL INJURY • Goal is to prevent rise in serum Cr and the need for renal replacement therapy. • Treatment of shock and hypovolemia • Restoration of adequate intravascular volume • 6-12 L of saline in first 24hrs is recommended • Urine flow rate of 100-200cc/hr is ideal • Correction of underlying cause of shock • Measure serial CK levels in high-risk patients • Treatment threshold 5000-30,000 U/L
PREVENTION OF RENAL INJURY • Alkalinization of urine with NaHCO3- (K+) • Mannitol • Dopamine, acetazolamide, and Lasix • Experimental therapies: • Deferoxamine • PAF-receptor blockade • Bosentan – endothelin receptor blockade • Anti-oxidants
Mannitol Mannitol Sodium Bicarbonate
Better OS, Stein JH. Early Management of Shock and Prophylaxis of Acute Renal Failure in Traumatic Rhabdomyolysis. New England Journal of Medicine 1990; 322 (12): 825-829 • Hypothesis: Shock occurs only after extrication, when compressed extremities are released, resulting in ischemia-reperfusion injury • 1979: 7 men with rhabdo due to building collapse who did not receive IV fluid for at least 6 hours; all 7 developed ARF • 1982: 7 men with traumatic rhabdo who received IV fluid before extrication and forced mannitol-alkaline diuresis within 2 hours of extrication; none developed ARF
SERUM CREATINE KINASE LEVELS $15 1-2 hour turnaround Elimination T1/2: 42 hrs More prevalent in the literature - >3000 pts Peak levels of 5000 to 75,000 risk ARD All pts with increased CK levels have positive urine dipstick** URINE OR SERUM MYOGLOBIN LEVELS $97 1-3 day turnaround Elimination T1/2: 12 hrs Studies with small numbers - <300 pts Most studies use urine levels which are affected by renal function TREATMENT THRESHOLD
DIALYSIS • Risk factors for developing ARF: • CK level >20,000 • Delay in diagnosis or treatment • Extent of injury • Dehydration • Preexisting renal disease • Advanced age • Administration of nephrotoxic agents • Normalization of Hyperkalemia is the main priority. • Need for dialysis is temporary in most cases
EARTHQUAKES AND RHABDOMYOLYSIS • 1988: Armenian Republic of Soviet Union • 100,000 injured, 15,254 extricated from rubble, crush injury third most common injury but leading cause of death, 323 patients required hemodialysis, poorly organized disaster response • 1991: Limon, Costa Rica • Crush injury was the leading cause of injury and death
EARTHQUAKES AND RHABDOMYOLYSIS • 1995: Kobe, Japan • 41,000 injured, 5000 died, 54% of victims with crush injury developed ARF and 13% died • 1999: Marmara, Turkey • Renal Disaster Relief Task Force created in 1995 after Armenian earthquake • 462 patients underwent dialysis, with <19% mortality rate (this was a dramatic improvement in the delivery of treatment and survival)
Oda et al. Analysis of 372 Patients with Crush Syndrome Caused by the Hanshin-Awaji Earthquake. Journal of Trauma 1997; 42: 470-476 • Retrospective review of 6107 charts at 95 hospitals; 372 patients with crush syndrome • ARF= Cr > 2.5; 200 (54%) ARF, 123 (33%) required dialysis • Many patients had a delay until treatment, either due to transportation problems or failure to accurately diagnose crush injury. • Risk factors for ARF: <6 L fluid / day, delay until treatment, and CK >75,000 • 50 patients died (13.4%); causes of death within 5 days of the earthquake were mainly hyperkalemia and hypovolemia.
Oda et al. Analysis of 372 Patients with Crush Syndrome Caused by the Hanshin-Awaji Earthquake. Journal of Trauma 1997; 42: 470-476 *black = hypovolemia, diagonal stripe = hyperkalemia, horizontal stripe = other form of shock, vertical stripe = multiple organ failure, open = other causes
Oda et al. Analysis of 372 Patients with Crush Syndrome Caused by the Hanshin-Awaji Earthquake. Journal of Trauma 1997; 42: 470-476 ***9% had trunk involvement; extremities do not need to be involved to develop rhabdomyolysis.
RECENT PUBLICATIONS AND UNPUBLISHED DATA FROM USC/LAC AND OHSU