Download
1 / 36
370 likes | 834 Views
Periprosthetic Fractures Adjacent to Total Knee Implants:. Decision making and Principles of Management ICL 49 & 50 Gerard A. Engh, MD Cecil H. Rorabeck, MD. Characteristics of Periprosthetic Fractures. Typically elderly with severe osteoporosis

E N D
Periprosthetic Fractures Adjacent to Total Knee Implants: Decision making and Principles of Management ICL 49 & 50 Gerard A. Engh, MD Cecil H. Rorabeck, MD
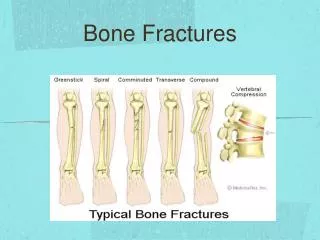
Characteristics of Periprosthetic Fractures • Typically elderly with severe osteoporosis • Usually medical complications associated with bed rest and inactivity • protected weightbearing often impossible because of multiple-joint involvement, neurological disorders, and systemic illness. • Periprosthetic Fxs may occur either intraoperatively or postoperatively
Intraoperative Periprosthetic Fractures of the Femur, Tibia, and Patella • Most fractures are neither displaced nor comminuted and the stability of the components is rarely altered and normally there is minimal soft tissue trauma. • Usually, screws are adequate for stabilizing the fx, and the patient may safely proceed with an unaltered rehabilitation protocol.
Femoral Fractures (neck) • Femoral neck fxs are a rare complication that are related to the force of femoral impaction. • This should be expected in patients who are slow to mobilize or who complain of hip and thigh pain after routine TKA.
Femoral Fractures (condylar and supracondylar) • Fractures that split the condyle while making the box cut for a posterior stabilized component can be stabilized by using a transcondylar cancellous bone screw • This is usually sufficient because the cement and femoral component provide additional support. • If the condyle is displaced or comminuted, the fx is best treated with a long-stemmed femoral component that stabilizes the condyle to the diaphysis.
Femoral Fractures (shaft) • Fractures of the anterior femoral cortex can occur when the cortex is perforated accidentally while the surgeon is inserting an intramedullary alignment rod. • A long-stemmed implant that bypasses the perforation should be used • Protected weightbearing is advisable for a minimum of 6 to 8 weeks.
Tibial Fractures (metaphyseal region) • Tibial fxs can be caused by impingement of the stem when impacting the implant with peripheral fins or pegs. • These are usually vertical in nature within the metaphysis. • Fixation of the tibial component with cement is generally satisfactory to protect the fx, however a cancellous bone screw can be placed for additional stabilization. • Activities should be modified in the early postop period.
Tibial Fractures (shaft) • Tibial shaft fxs can occur with impingement of the stem into the diaphysis. • Fxs of the middle third of the tibia are best treated with a patellar ligament-bearing cast that permits knee flexion. • Fxs of the proximal third of the tibia require additional support proximal to the knee with a cast or brace for a period of 3 months.
Tibial Fractures (tibial tubercle) • More common when the knee range of motion is significantly restricted before surgery. • Usually occurs with initial patellar eversion and flexion of the knee. • Should be repaired with screws or tension wires and reinforced with soft-tissue repair and postop splinting. • Active quadriceps activity should be avoided for 6 weeks.
Patellar Fractures • Usually the result of removal of a stable patellar implant from osteoporotic bone at the time of revision. • Vertical fxs are usually stable and require no internal stabilization. • Transverse fxs can interrupt the integrity of the extensor mechanism and should be stabilized with the tension-band-wire technique to permit early ROM.
Patellar Fractures cont. • The patellar component should not be reimplanted if the fractured patella requires surgical repair. • If satisfactory stability cannot be obtained with flexion to 90 degrees, the fx fragments should be excised and a repair of the extensor mechanism should be augmented.
Postoperative Periprosthetic Femoral Fractures • Incidence ranges from 0.3% to 2.5% (meta-analysis) • Predisposing factors are common features. • Revision arthroplastly has a higher incidence than primary. • Anterior notching has been implicated by some authors. • Restricted range of flexion in the replaced knee also increases the risk of fx.
Supracondylar periprosthetic Fracture Classification • The modified Neer classification • Type I: extraarticular and nondisplaced supracondylar fractures--prosthesis stable. • Type II: extraarticular with displacement of greater than 5mm or 5 degrees of angulation--prosthesis stable. • Type III: severely comminuted with loss of cortical contact and significant angulation--prosthesis loose or failing.
Type I Femoral Fractures • If a type-I fracture is stable and the prosthesis is intact and functioning well, and the patient can walk safely while wearing a cast or cast-brace, then the knee is best treated closed and with ROM exercises. • The patient must have enough strength to walk safely with protected weightbearing until the fracture has healed for at least 6-8 weeks.
Type I cont. • Surgical intervention is necessary to stabilize an undisplaced type-I fracture in patients who cannot tolerate a cast or cast-brace or remain partial weightbearing. • Intramedullary fixation devices are ideal because they minimally disrupt the fracture hematoma. • Examples include: Rush rods, Zickel supracondylar rods, retrograde nails.
Type I cont. • An other option includes a blade-plate--this requires considerably more dissection and periosteal stripping in the region of the fracture. • Early knee motion is necessary to optimize the functional results of nonsurgical treatment of type-I fxs.
Type II Femoral Fractures • Surgical intervention is indicated for type-II supracondylar fxs that have resulted in unacceptable alignment of the extremity or the components. • Variables to consider when selecting a fracture-fixation device include displacement and angulation, alignment of the extremity, bone quality, bone deformity, and the type of knee implant that is in place.
Type II Femoral Fractures-treatment options • Plate-and-screw fixation • External fixators • Supracondylar Intramedullary Rods
Plate-and-Screw fixation • With plate-and-screw fixation, the condylar fragments must be large enough and of sufficient bone density to provide rigid distal fixation. • Buttress plates offer the greatest flexibility but the are the least secure. • A blade-plate is usually the best of the plate-and-screw fixation for comminuted distal condylar fxs. • Bone graft or cement may also be used.
External Fixators • Have been used successfully but are usually contraindicated in the treatment of supracondylar fxs. • Because the fixator cannot cross the joint the pins are placed close to the prosthesis and risk infecting the joint via the pin sites. • The pins also impede the quadriceps muscle and affect ROM.
Supracondylar Intramedullary Rods • Available in lengths of 15, 20, 25 cm.--best to use the longest rod because it centers itself in the isthmus and decreases the risk of fx malalignment. • The type of prosthesis must be identified to determine if the intercondylar notch is wide enough to accommodate insertion of a supracondylar rod. No PSFC’s. • A minimum distance of 12mm is necessary.
Type III Femoral Fractures • Treatment can be performed one of two ways: like a type-II fracture, with revision of the implant at a later date, or with revision of the implant as part of the fracture stabilization. • If a revision is performed, a long-stemmed implant, a custom-made component, a tumor prosthesis, or an allograft-implant composite should be used.
Type III cont. • A stable tibial component can be retained if the femoral component is of the same design. • Dome-shaped patellar components should not be revised as they articulate satisfactorily with most femoral components. • It is prudent to have an implant or an allograft available that will replace damaged bone of the femoral condyles if necessary.
Type III-early revision • Early intervention and revision of the femoral component to one with a canal-filling stem are the best options for treatment of type-III fxs. • It is important to keep cement away from the fx site whenever possible as this will delay or prevent healing.
Type III-delayed revision • The exceptional patient who should not have early intervention is one who will benefit from delayed revision. • Two advantages to delaying revision: • 1. Revision of an anatomically healed fx is far easier than one with unstable condylar fragments. • 2. A standard revision implant can be used which have a greater chance of long-term stability.
Complications • Chen and associates stated that the complication rate for both surgical and nonsurgical intervention is about 30%. • Complications include: nonunion, malunion, infection, and knee stiffness. • If rigid internal fixation is achieved, early motion with CPMs and physical therapy is beneficial.
Tibial Fractures • Periprosthetic fxs of the tibia are relatively uncommon. • Predisposing factors for tibial fracture are similar to those for the femur • The integrity of the prosthetic fixation and the bone quality are the primary factors deciding the appropriate treatment option.
Tibial Fractures-fixed prosthesis • If the prosthesis is fixed and the fracture pattern stable and in good alignment, closed techniques can be performed. A long-leg cast, followed by a hinged cast brace should maintain the position. • Protected weightbearing for at least 6 weeks is advised.
Tibial Fractures-loose prosthesis • Revision should be performed if the prosthesis is loose. Use of stemmed components with or without bone grafting is the treatment of choice.
Patellar Fractures • Patellar fractures are the most frequent periprosthetic fractures encountered with TKA. • Usually traumatic or stress fxs, with the latter being more common. • Predisposing factors similar to supracondylar fxs, however, there is an increased incidence in males and active patients, and excessive ROM in the early postop period.
Patellar Fractures-cont. • Deep central pegs and press-fit cementless components also are believed to increase fx risk. • Technical factors such as excessive bone resection or resurfacing of thin patellae (<13mm) are predisposing factors, along with revision surgery, heat necrosis from cement, and patellar devascularization.
Patellar Fractures-classification • Type-I Extensor mechanism intact, not extending into the implant interface • Type-II Extensor mechanism disrupted or extension to implant interface • Type-III Inferior pole fracture, patellar ligament rupture, or patellar ligament intact • Type-IV Associated patellar dislocation
Patellar Fracture-nonsurgical treatment • Stable prosthesis with intact extensor mechanism can usually be treated with a cylinder or long-leg cast. Vertical fxs can begin early ROM exercises. • Even comminuted posttraumatic fractures that do not disrupt the extensor mechanism and, as long as the component is stable, can be managed nonsurgically. Insall recommends 6 weeks in a plaster cylinder with full weightbearing for these fractures.
Patellar Fracture-surgical treatment • Fractures that produce significant extensor lag or are displaced by more than 2cm should be repaired. Tension band wiring or use of lag screw are the techniques of choice and the repair should be protected postoperatively as for any patellar fx. • If the component is loose, removal without replacement should be performed because of the unreliable refixation of the component with a healing fx.
Patellar Fracture-surgical treatment cont. • In severely comminuted fractures or those producing maltracking of the fragments, patellectomy is sometimes required. • Immobilization of a TKA for 6 weeks may lead to slight decrease in the overall knee score; however, final ROM and need for walking aids is not significantly changed. • Extensor disruption or patellar dislocation does lead to significant loss of ROM and need for walking aids.
Conclusion • Periprosthetic fxs represent difficult management problems in most cases. • The decision whether or not to perform surgery will be based on the location and displacement of the fx, fixation and stability of the prosthesis, and the quality of the bone around the fx and prosthesis. • Algorithms provide a general guide to treatment, but the needs of the individual will dictate the final choice and outcome.