Download
1 / 1
20 likes | 256 Views
No. 092. Active s urveillance in prostate c ancer - A New Zealand tertiary centre’s experience. Omid Yassaie, Farrael Mohd Azmin , Rod Studd Wellington Hospital, New Zealand. Posters Proudly Supported by:. Introduction

E N D
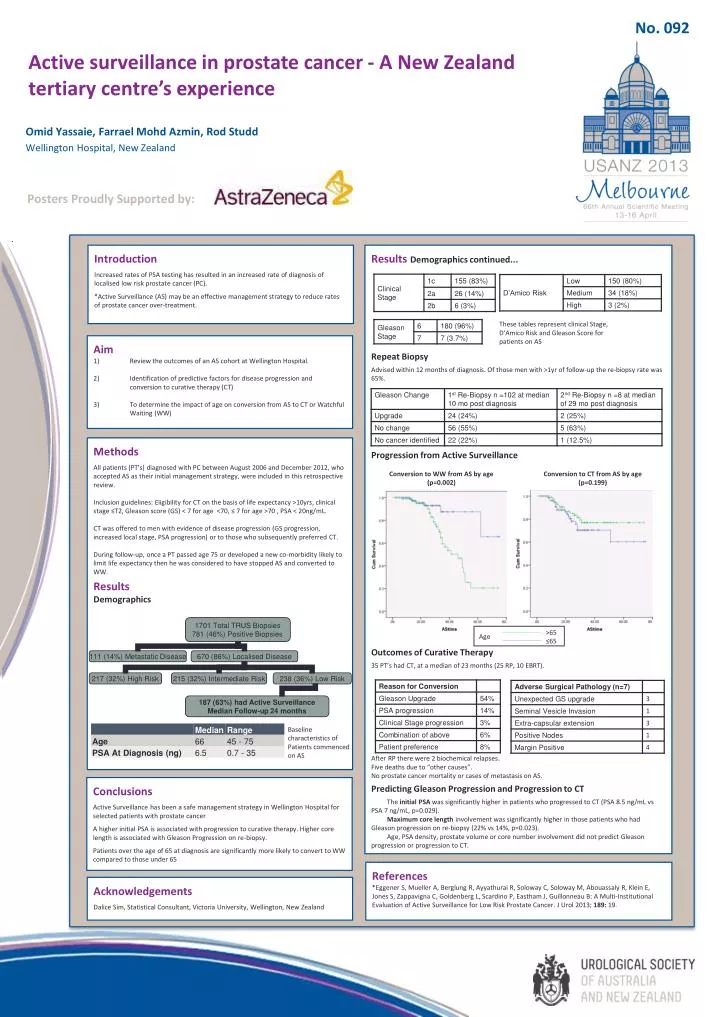
No. 092 Active surveillance in prostate cancer - A New Zealand tertiary centre’s experience Omid Yassaie, FarraelMohdAzmin, Rod Studd Wellington Hospital, New Zealand Posters Proudly Supported by: Introduction Increased rates of PSA testing has resulted in an increased rate of diagnosis of localised low risk prostate cancer (PC). *Active Surveillance (AS) may be an effective management strategy to reduce rates of prostate cancer over-treatment. Results Demographics continued... Repeat Biopsy Advised within 12 months of diagnosis. Of those men with >1yr of follow-up the re-biopsy rate was 65%. Progression from Active Surveillance Outcomes of Curative Therapy 35 PT’s had CT, at a median of 23 months (25 RP, 10 EBRT). . After RP there were 2 biochemical relapses. Five deaths due to “other causes”. No prostate cancer mortality or cases of metastasis on AS. Predicting Gleason Progression and Progression to CT The initial PSA was significantly higher in patients who progressed to CT (PSA 8.5 ng/mL vs PSA 7 ng/mL, p=0.029). Maximum core length involvement was significantly higher in those patients who had Gleason progression on re-biopsy (22% vs 14%, p=0.023). Age, PSA density, prostate volume or core number involvement did not predict Gleason progression or progression to CT. These tables represent clinical Stage, D’Amico Risk and Gleason Score for patients on AS • Aim • Review the outcomes of an AS cohort at Wellington Hospital. • Identification of predictive factors for disease progression and conversion to curative therapy (CT) • To determine the impact of age on conversion from AS to CT or Watchful Waiting (WW) Methods All patients (PT’s) diagnosed with PC between August 2006 and December 2012, who accepted AS as their initial management strategy, were included in this retrospective review. Inclusion guidelines: Eligibility for CT on the basis of life expectancy >10yrs, clinical stage ≤T2, Gleason score (GS) < 7 for age <70, ≤ 7 for age >70 , PSA < 20ng/mL. CT was offered to men with evidence of disease progression (GS progression, increased local stage, PSA progression) or to those who subsequently preferred CT. During follow-up, once a PT passed age 75 or developed a new co-morbidity likely to limit life expectancy then he was considered to have stopped AS and converted to WW. Results Demographics Conversion to WW from AS by age (p=0.002) Conversion to CT from AS by age (p=0.199) >65 ≤65 Age Baseline characteristics of Patients commenced on AS Conclusions Active Surveillance has been a safe management strategy in Wellington Hospital for selected patients with prostate cancer A higher initial PSA is associated with progression to curative therapy. Higher core length is associated with Gleason Progression on re-biopsy. Patients over the age of 65 at diagnosis are significantly more likely to convert to WW compared to those under 65 References*Eggener S, Mueller A, Berglung R, Ayyathurai R, Soloway C, Soloway M, Abouassaly R, Klein E, Jones S, Zappavigna C, Goldenberg L, Scardino P, Eastham J, Guillonneau B: A Multi-Institutional Evaluation of Active Surveillance for Low Risk Prostate Cancer. J Urol 2013; 189: 19. Acknowledgements Dalice Sim, Statistical Consultant, Victoria University, Wellington, New Zealand