Download
1 / 74
740 likes | 951 Views
Prostate cancer diagnosis, screening, management options and complications and myths of treatment

E N D
Screening for Prostate Cancer Mr M Saqib MRCS, MSc (Urol), FRCS (Urol)
• PROSTATE CANCER most common cancer in men • Survival rates have increased • Increased number of men now living with aftermath of disease and treatment • Limited support and awareness provided for MEN to help themcope with the disease and its treatment
Richard J. Ablin, PhD, DSc (Hon),
PSA: The Great Prostate Mistake • Ablin, New York Times March 2010 • 16% of American men diagnosed with prostate cancer; 3% die of it • ‘I never dreamed that my discovery four decades ago would lead to such a profit- driven public health disaster’ • 22% of men with normal (low) PSA have cancer
The Prostate Pyramid Death from prostate cancer (3%) Diagnosed prostate cancer (15%) Men with prostate cancer (50%) All Men (100%)
CANCER – WORLDWIDE BURDEN (2005) 11 million New Cases 7 millionDeaths 25 millionLiving with Cancer
CANCER – WORLDWIDE BURDEN (2030) 27 million New Cases 17 millionDeaths 75 millionLiving with Cancer
U.S. Health Care Spending In 2009, the U.S. spent $2.53 TRILLION on Health Care
• I wonder if I should be getting my prostate checked out? • Or, I go to pee more often? • What are my chances of cancer? Should I be worried?
Risk Factors • Age • Family History • Ethnicity • Diet: • Cooked and processed tomatoes better than fresh • ▪European Investigation into Cancer and Nutrition (EPIC) study - positive (three other studies showed no association) • Calcium and dairy products: The EPIC study showed increased risk from dairy protein and dairy calcium. • Fat and meat: inconsistent • Fruit and vegetables: EPIC: no association with total fruit and vegetable intake Green tea (polyphenols) and
Acquired risk factors • Alcohol and smoking: Two meta-analyses: not linked • Obesity and physical activity: A recent meta-analysis reported a small borderline increase with BMI • NSAIDs - Several meta-analyses show aspirin reduces the risk • Statins – not in short-term! Vasectomy - marginal increase, 1.07 RR at 10 years, selection bias.
Efficient Health System • Some consume too much (Unnecessary care given) • Some consume too little (Necessary care not given) • We could decrease the waste and improve overall health! • Evidence Based Medicine
Cancer Death Rates* by Sex, US, 1975-2006 Rate Per 100,000 Men Both Sexes Women *Age-adjusted to the 2000 US standard population. Source: US Mortality Data 1960-2006, National Center for Health Statistics, Centers for Disease Control and Prevention, 2009.
Breast Cancer (Taskforce Estimates) • One year of screening women aged 40 to 49 • 22,327,000 women screened • 32,000 diagnosed • 24,200 survive • 7800 deaths • 1200 lives saved by mamography
Prof. David Forman • For many of the types of cancer that we looked at that affect both sexes, there’s no known biological reason why men should be at a greater risk than women, so we were surprised to see such consistent differences….. Men have a reputation for having a ‘stiff upper lip’ and not being as health conscious as women.” Professor David Forman (2009) NCIN
Treating Men » Men are less likely than women to utilise psychological support services » Men are low users of cancer information services » Current prostate support groups poorly attended
Cont. • Voluntary groups expressed difficulty in recruiting and retaining men on their programmes • However, men do care about their health and want to be pro-active in collaboration with HCPs
Consultation for PSA • Fear of cancer • Consequences (anxiety) of living with insignificant cancer. • Impact of Rx on QoL • Current lack of scientific proof of Rx.
Benefits of PSA • Early detection • Could extend life if high grade cancer detected.
Wilson and Junger Criteria 1969 3. Accurate diagnostic test (and acceptable, cheap)
Wilson and Junger Criteria 1969 1. Significant burden of particular disease in the community 30, 000 new cases/yr 10,000 deaths/ yr Lifetime risk of 18% (doubled in PSA era) Lifetime risk of death PCa 3% Commonest cancer and 2nd leading cause of death in men 2. Natural history of disease should be known Studies available on the natural history of non-screen detected PCa but we do not know the natural history of screen detected cancer – does screening result in a lead time bias?
Wilson and Junger Criteria 1969 4. Effective or useful treatment should be available for early stage disease Controversy as to whether radical treatments result in longer survival Evidence stems from Bill-Axelson A, Holmberg L et al 2005 NEJM
Prostate Cancer Screening Studies European Randomized Study of Screening for Prostate Cancer Schroeder FH et al 2009 NEJM: • 162,387 men 55-69 yrs randomised to receive PSA screening every 4 yrs or no PSA screening in 7 European countries • Prostate cancer diagnosed in 5,990 (8.2%) of screened group and 4,307 (4.8%) of control group • After median FU of 9 years there were fewer cancer deaths in screened group (214 vs 326) • 1,410 patients have to be screened to prevent 1 cancer death and 48 screened men would have to be treated to prevent 1 death • Therefore although screening did reduce mortality there was high risk of overdiagnosis and screening would not have as much effect as we would have hoped
Wilson and Junger Criteria 1969 However, PSA is prostate specific but not prostate cancer specific. Raised in many other situations What is normal PSA? Either absolute value 4ng/ml or age dependent: Osterling’s age specific reference range Age PSA(ng/ml) 40-50 2.5 50-60 3.5 60-70 4.5 70-80 6.5
Wilson and Junger Criteria 1969 5. Long latent period 6. Availability of health and resources 7. Economic implications
> RRP increases overall survival, relative to watchful waiting, in men with clinically detected prostate cancer. >For all end-points the advantages have increased over time and expected that may increase further with longer FU
Prostate Cancer Screening Studies US study - the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial Andriole GL et al NEJM 2009: •Concluded that after 7 to 10 years of follow-up the rate of death from prostate cancer was very low and did not differ significantly between the two study groups
More Specificity of PSA PSA derivativeNormal PSA velocity <0.6 - 0.75ng/ml/year *PSA doubling time More than 3 years PSA density <0.15ng/ml/ml PSA transitional zone density <0.35ng/ml/ml Free to total PSA >20% *Supersensitive PSA <0.01ng/ml
Prosdex • Web based decision on www. Prosdex.com/index_content.htm
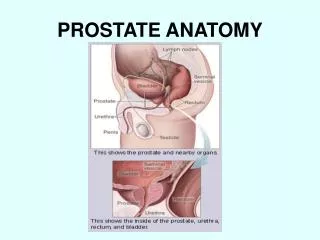
Current attribution of prostate cancer status Serum marker Men at risk by age Histological phenotype Men at risk by PSA or DRE Examination for extracapsular disease Pathological verification Potential for overtreatment
What is wrong with the current pathway? Low PPV Cannot exclude disease Random and systematic error (1/3 upgrade at RP) Instability of cancer status Detects indolent disease Biopsy artefact Only applied when TRUS positive High NNT in screen detected cancer Cost Morbidity
The prostate cancer journey... for most people MRI for staging suspicion biopsy treatment follow up surveillance
The prostate cancer journey... new possibilities MRI to detect cancer 1 suspicion better biopsy treatment follow up 50%? better surveillance 1. MRI for detecting caner: a) improve the biopsy b) eliminate post biopsy haemorrhage artefact c) eliminate biopsy in some
The prostate cancer journey... new possibilities MRI to plan treatment MRI to detect cancer 1 3 suspicion better biopsy treatment follow up 50%? MRI to detect change in cancer volume or grade 2 better surveillance 3. MRI to plan treatment: a) plan margins b) plan focal therapy
The prostate cancer journey... new possibilities MRI to monitor for recurrence MRI to asess completeness of treatment MRI to plan treatment MRI to detect cancer 1 3 suspicion better biopsy treatment follow up 50%? MRI to detect change in cancer volume or grade 2 better surveillance 4 & 5 MRI to asess treatment & monitor for recurrence
Background - 4 Prostate Mapping Biopsies Approximate 90-95% accuracy in detection of significant disease (Beware: computer simulation!) 0 Crawford et al, 2005; Barzell et al, 2007; Pinkstaff DM et al, 2005; Satoh et al, 2005; Merrick et al, 2007
Gleason Grade Benign glands Gleason grade 3 Gleason grade 5
MR post needle – 2 /12 PREBX 6 / 12 2 WEEKS
Incidence of nodal metastases T1/T2 < 5% Early T3 15% T3 30% T4 >40%