Download
1 / 27
280 likes | 482 Views
Liver Trauma . Mohamed. Hashim Milhim 4th year medstudent An-najah national univ. Background. Largest organ, 2nd most common injured, Blunt trauma most common. Why the liver…. Friable parenchyma, thin capsule, fixed position in relation to spine prone to blunt injury .

E N D
Liver Trauma Mohamed. Hashim Milhim 4th year medstudent An-najah national univ.
Background • Largest organ, • 2nd most common injured, • Blunt trauma most common
Why the liver… • Friable parenchyma, thin capsule, fixed position in relation to spine prone to blunt injury . • Right lobe larger, closer to ribs. more injury • In children compliant ribs, transmitted force
Mechanisms of injury:- • simple compression against ribs, spine, • ligamentous attachment to diaphragm and the posterior abdominal wall ,shear forces during deceleration injury.
Mechanisms of injury:- • High-velocity bullet injuries • burst injuries with distant contusions and parenchymal disruption. • Associations
Mechanisms of injury:- Low-velocity penetrating injury • Stab wounds • percutaneous biopsy • cholangiography • biliary drainage, • (TIPS), • capsular tears, hematoma, bile leaks, arteriobiliary fistulas, and hemoperitoneum, arterial aneurysms.
Associations: • Isolated liver injury occurs in less than 50% of patients. • Blunt trauma 45% with spleen • Rib fracture 33% with Liver injury
Injuries • Parenchymal damage • Subcapsular hematoma • Laceration • Contusion • Hepatic vascular disruption • Bile duct injury
Injuries • Mild injuries heal in 3 months. • Moderate injuries heal in 6 months. • Sever injuries in 9-15 months.
Clinically • Symptoms & signs of injury are • blood loss, • peritoneal irritation, • RUQ tenderness, and guarding. • delayed abscess . • Signs of blood loss may dominate the picture. • Biliary peritonitis.
Labs & Radiology • Elevated LFTs • DPL -- high sensitivity • CT scan is the diagnostic procedure of choice. • US. • MRI ??
Angiography • active bleeding • Transcatheter embolization • Embolization & stenting for fistulas.
CT Scan • Localization. • monitor healing. • Grades 1-6
Classification(AAST) I-Subcapsular hematoma<1cm, superficial laceration<1cm deep.
II-Parenchymal laceration 1-3cm deep, subcapsular hematoma1-3 cm thick.
III-Parenchymal laceration> 3cm deep and subcapsular hematoma> 3cm diameter.
IV-Parenchymal/supcapsular hematoma> 10cm in diameter, lobar destruction,
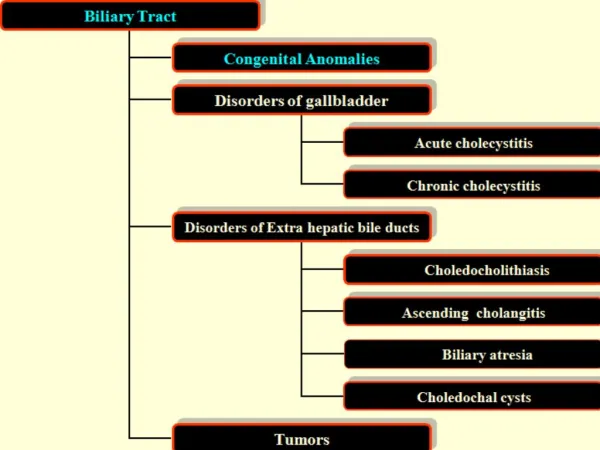
Gallbladder injuries… • Rare • Predisposing factors. • contusions, avulsions, lacerations or perforations.
Management • In the past VS now treatment of blunt liver injury trauma • 86% , 67% • CT scan diagnosis and follow up
Management… • Remember associated injuries • Resuscitate • Assessment of injury Spiral CT Laparotomy • Treatment
Management… • consider Cryoprecipitate, FFP • Rooftop incision • Control blood Loss
Suturing of Lacerations • Resection • Packing • Recurrent parenchymal bleeding transcatheter embolization