Download
1 / 25
250 likes | 464 Views
Underwriting Eye Disorders . Philippine Society of Insurance Medicine Updates. Eye Exam. Eye Exam – valuable information about the client. Classification: Purely local disorders of the eyes (conjunctivitis and other infections, ocular injuries, )

E N D
Underwriting Eye Disorders Philippine Society of Insurance Medicine Updates
Eye Exam Eye Exam – valuable information about the client. Classification: • Purely local disorders of the eyes (conjunctivitis and other infections, ocular injuries, ) • Manifestations of systemic disease (Diabetes Mellitus, hypertension, SLE, RA, Dermatomyositis, Hyperthyroidism)
Blindness – Most important ocular medical impairment that merits our underwriting attention. – Most important factor to be considered in risk assessment – its CAUSE. Mortality is increased when blindness is due to diabetic and hypertensive retinopathy and other causes where the primary disease itself is subject to extra mortality, than those that do not pose hazard to life, e.g. temporary ocular inflammatory conditions.
Blindness (MIRA) Total blindness Life CI TPD WPD ADB Unilateral 0 Excl Excl Excl 1 Bilateral 0 Excl Excl Excl Excl Partial blindness – Reduction of Visual Acuity Mild 0 0 1 1 1 Moderate 0 Excl Excl Excl Excl
Visual Acuity Reduction of visual acuity is a combination of reduced vision of both eyes. Confirms eye function? a) an optometrist b) an optician c) the agent d) an ophthalmologist e) the medical director
Optometrist – is a healthcare professional who performs routine eye examinations, administers primary eye care and prescribes eye wear – eyeglasses or contact lenses to improve vision. – is an O.D. (doctor of optometry)
Ophthalmologist – a specialist who has trained further or specialized in the diagnosis and treatment (medical or surgical) treatment of eye disorders. – is a medical doctor (M.D.)
Eye Report What should it contain? a) Nature and cause of the visual impairment b) Severity of the condition c) Both
Hypertensive Retinopathy Poorly controlled hypertension can give rise to hypertensive retinopathy (fundus hypertonicus). Grading – based on changes that occur in the blood vessels at the back of the eye which are correlated closely to the changes generally observed in blood vessels.
Hypertensive Retinopathy Positive Features: Grade I – II Well controlled BP Negative Features: Grade II – IV Poorly controlled blood pressure Impaired vision
Effect of hypertension on the retina Retinal changes: Grade 1 – mild narrowing or sclerosis of retina arteries Grade 2 – moderate to marked narrowing/sclerosis w/ light reflex and A-V crossing changes Grade 3 – w/ addtl. hemorrhages or cotton-wool spots Grade 4 – w/ addtl. swelling of the optic disk or papilledema
Hypertensive Retinopathy (MIRA Underwriting Guidelines) Life CI TPD WP ADB Grade 1 0 0 1 1 1 Grade 2 25 50 1.25 1 1 Grade 3 50 50 + Excl Dec Dec 1 Grade 4 Dec Dec Dec Dec Dec
Hypertensive Retinopathy An asymptomatic 58 yr-old businesswoman, FA 5M, hypertensive since 1998, BP = 140/90, w/ incidental finding of mild retinal artery narrowing in the eyegrounds; Past hx = adequately treated for papillary CA, thyroid, 20 yrs ago; no recurrence of disease; CXR normal, ECG = LVH, 2-D echo IVS = 11 mm, very minimal MR. Carotid doppler no stenosis; Chol 215 mg/dl, taking felodipine, simvastatin and Aspilet. What is your underwriting decision? a) Accept as substandard risk b) Postpone c) Decline d) Talk to the agent
Prevention of Hypertensive Retinopathy The most important element is the achievement of satisfactory blood pressure control.
Diabetic Retinopathy Long-term complications of diabetes – due to accelerated vascular disease. Smaller vessels are affected, most noticeable in the retina, called RETINOPATHY – Initially, non-proliferative (small vessels break and leak), and then proliferative (blood vessels abnormally grow in the retina producing scarring, leading to retinal detachment and loss of vision.)
Diabetic Retinopathy What do you need: a) FME, MUR b) Diabetes questionnaire c) BEX (blood exam) – FBS, HbA1c, OGTT where needed Reminder: HbA1c is not recommended for the diagnosis of diabetes; it is best used to monitor long term control and prognosis of this disease.
Diabetic Retinopathy (MIRA) Life CI TPD WP ADB Visual impairment Dec Dec Dec Dec Dec caused by diabetic retinopathy
Diabetic Retinopathy (Brackenridge) Basic Ratings for NIDDM: 31 – 40 yrs old +100 41 and above +50 Additional Ratings for retinopathy Mild (microaneurysms) 0 Moderate (exudative) +50 Severe (proliferative) +100
Diabetic Retinopathy (Brackenridge) Proteinuria Trace 0 +1 +50 +2 +100 +3 and up Decline Smoker – additional +50
Diabetic Retinopathy 60 yr-old male executive, nicotine addict 10 sticks/day FA 2M, diabetic for the past 10 yrs, has irreg. intake of Euglucon, sees “floaters”, eyegrounds show some microaneurysms and exudates; last ff up with his endocrinologist 2 yrs ago. HbA1c = 9.4; FBS = 118 mg%. MUR shows +2 proteinuria, ECG – normal What is your underwriting action? a) accept as highly substandard risk b) postpone c) decline d) talk to the agent
Prevention of Diabetic Retinopathy If the incidence and severity of diabetic complications are to be avoided, it is imperative that blood sugar level be maintained within normal levels.
Uveitis Life CI TPD WPD ADB Present 0 Excl Excl Excl 1 In history 0 0 1 1 1
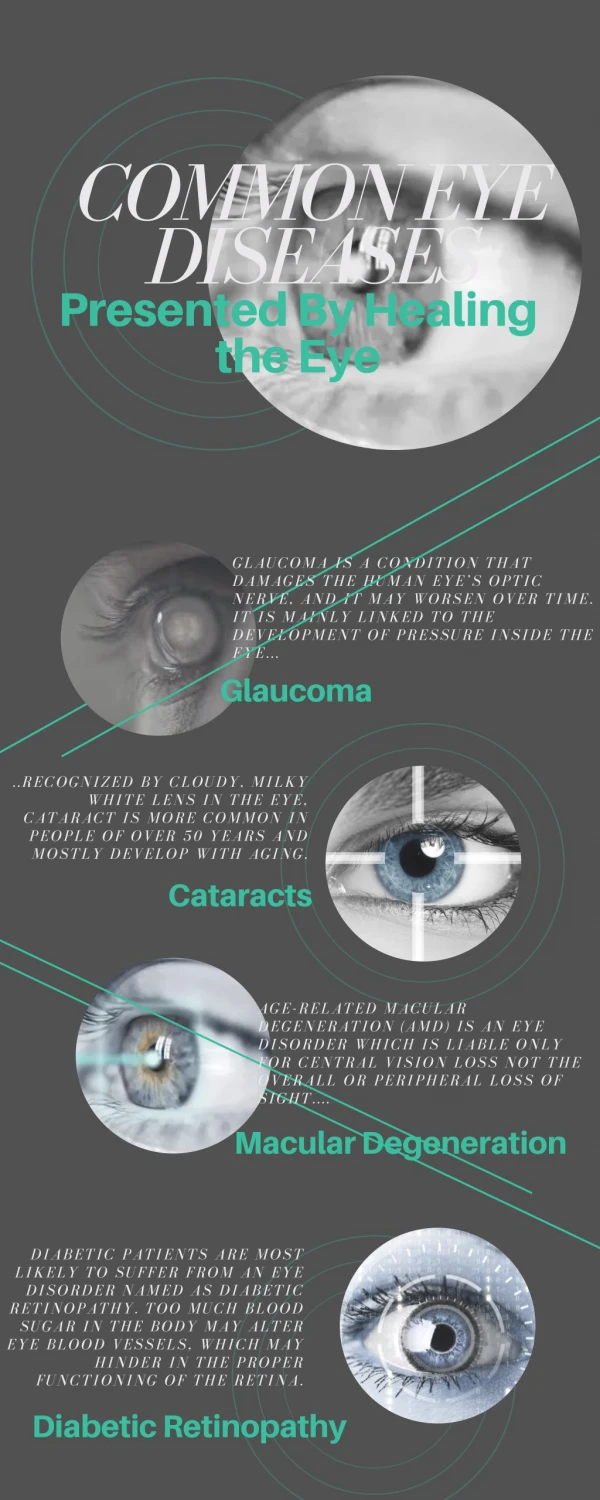
Glaucoma Causes: Uveitis, intraocular trauma, use of steroid eye drops, rubeosis in diabetes MIRA Guidelines W/ visual impairment – Standard, ADB W/o visual impairment stable – standard, w/ CI, ADB unstable – standard, ADB
Cataract • Lens opacity, usually age-related • Diabetic causes • Others: trauma, systemic steroid use, congenital, occupational Life CI TPD WPD ADB Operated 0 Excl Excl Excl 1 Unoperated 0 Excl Excl Excl 1