Download
1 / 57
630 likes | 970 Views
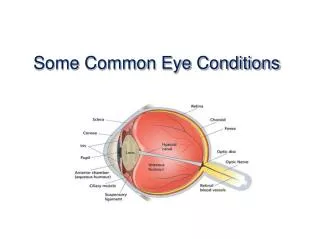
Common Eye Disorders. Dina Mohammed Abdulmannan Umm Al-Qura university. Chalazion. Chalazion. Inflammation of a meibomian gland Also called an internal hordeolum Usually requires no treatment, although if persistent may require surgical excision

E N D
Common Eye Disorders Dina Mohammed Abdulmannan Umm Al-Qura university
Chalazion • Inflammation of a meibomian gland • Also called an internal hordeolum • Usually requires no treatment, although if persistent may require surgical excision • Hot compresses may be tried to help unblock meibomian gland
Blepharitis • A common, chronic, inflammatory condition of the eyelid margins • Signs: • waxy, shiny lid margins • oily/debris in tear film • itchy, irritated eyes • most common cause of dry eye
Blepharitis • Treatment: • Eyelid hygiene is the mainstay of treatment. This helps to remove crusts/scales and helps unplug blocked meibomian glands • Warm compresses and eyelid massage • Natural tears give some relief, don’t cure problem • Occasionally AB’s for staphylococcal blepharitis
Conjunctivitis • Inflammation of the conjunctiva • Signs: • redness • swelling • discharge • grittiness
Conjunctivitis • Often viral infection • Treatment is dependant on the cause. May be: • viral • bacterial • allergic • follicular • others
Corneal Abrasion • Scraped area of corneal surface, accompanied by loss of epithelium. • Abrasions of the epithelium heal within 72 hours and do not leave a scar. Deeper lesions, involving Bowman’s layer and below, heal with permanent opaque scarring.
Corneal Abrasion • Treatment may be with artificial tears for a minor abrasion or patching/bandage contact lens (BCL) application for more severe abrasions
Keratoconus • Degenerative corneal disease • Characterized by generalized thinning and cone-shaped protusion of the central cornea • Typically bilateral • Usually diagnosed in the second decade
Keratoconus • Causes increase in myopia, astigmatism and surface irregularity • In early stages, glasses or soft contact lenses may be used • As disease progresses, need to use hard contacts to provide smooth refractive surface. • Advanced cases may require penetrating keratoplasty
Corneal Graft(Penetrating Keratoplasty) • Replacement of a scarred or diseased cornea with clear corneal tissue from a donor. • Usually reserved for severe cases, where there is a good chance of vision improving after surgery
Cataract • Any lens opacity • May be classified by age (congenital to senile), stage (early to hypermature), or type (NS, cort, PSC, etc) • Some systemic diseases/conditions predispose to cataract (DM, RA, hypothyroid, smoking, corticosteroid use, etc)
Cataract • Treatment: • always the same regardless of what type or stage of cataract. • CE with placement of either a AC or PC IOL. The power of the lens used is determined by the length of the eye (A-scan measurement) • Phacoemulsification is used (US) to break up the cataract and remove it from the eye. Uses much smaller incision then removal of whole lens. Shorter healing time, less chance of infection, etc.
Post Cataract Surgery • Posterior capsule opacification (PCO) • a membrane that forms behind the IOL causing a decrease in vision. • may see Elschnig pearls on retroillumination • treatment is with a capsulotomy
Glaucoma • An optic neuropathy with characteristic optic nerve head changes • Diagnosis is determined by ON evaluation, IOP measurements, and visual field findings.
Glaucoma • Normal findings: • ON: cup to disc ratio (c/d) of 0.4 or less • IOP: 10-21 mm Hg for average corneal thickness • VF: full field (no paracentral scotomas, diffuse depression, nasal steps or arcuate scotomas)
Glaucoma • Treatment: • topical or oral medication (many different types) • laser surgery • incisional surgery
Iritis • Inflammation of the iris • Signs: • red eye • pain • tearing • blurred vision • miosis (small pupil)
Iritis • Cause is unknown • Iritis is graded at the slit lamp based on the presence of cells and flare in the AC • Associated with systemic inflammatory conditions (RA, SLE, etc) • Treatment is with dilating drops and topical steroids to reduce inflammation • Often have recurrent flare-ups
Uveitis • Inflammation of the uvea (iris, ciliary body, choroid) • Anterior uveitis (iridocyclitis) - iris or ciliary body • Posterior uveitis - choroid
Uveitis • Signs: • photophobia • decreased vision • small pupil (meiosis) • red eye (usually most prominent at limbus) • normal IOP
Uveitis • Treatment is with topical steroids • Steroids help to prevent secondary problems (cataract, uveitic glaucoma, adhesions of iris to lens) • In severe cases, systemic steroids may be required • Recurrence is common
Posterior Vitreous Detachment (PVD) • Separation of the vitreous gel from the retinal surface • Tends to occur with aging as the vitreous liquifies • May also occur in the presence of high myopia and diabetes
Posterior Vitreous Detachment (PVD) • No treatment is required in most cases • Floaters tend to become less bothersome over time • Treatment is required if there are retinal tears associated with the PVD which may lead to retinal detachment
Diabetic Retinopathy (DR) • Spectrum of retinal changes that accompany long-standing diabetes mellitus • Early stage is non-proliferative (dot and blot hemmorhages, hard exudates, microaneurysms) • May advance to proliferative (neovascularization and fibrous tissue) if blood sugars not controlled
Diabetic Retinopathy (DR) • Treatment of proliferative disease is with panretinal laser photocoagulation (PRP) • Concept of treatment is that areas that are scarred require less oxygen, therefore, this should promote regression of new blood vessels (neovascularization)
Retinal Detachment (RD) • Separation of sensory retina from underlying pigment epithelium • May be caused by a retinal tear or by fibrous tissue traction • Symptoms are flashing lights, streaks of lights, curtain coming across the eye, loss of vision
Retinal Detachment (RD) • Treatment is surgical and is usually done immediately • A scleral buckle may be used in some cases