Download
1 / 34
341 likes | 712 Views
Introduction. The choice of ventilator settings

E N D
1. Initial ventilator settings Dr Chaitanya Vemuri
Int.Med M.D Trainee
2. Introduction The choice of ventilator settings � guided by clearly defined therapeutic end points.
In most of cases : primary goal is to correct abnormalities of arterial blood gas tensions
Accomplished by
adjusting minute volume - to correct hypercapnea
oxygen supplementation � to correct hypoxemia
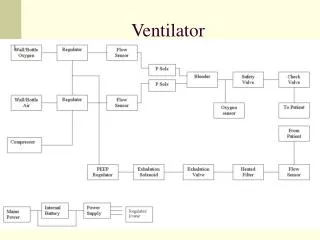
3. General aspects of ventilator management
Choice of inspired gas composition
Means to ensure the machine�s sensing of patient�s demand
Definition of machine�s mechanical output
4. INITIATION
5. Confirm indication for mechanical ventilation
Invasive / Non invasive
Check Connections & Circuit
Self test
Select mode
Set variables
Alarm settings
Connect to patient
Monitor and reassess
6. indications Patient not breathing
Patient breathing but not enough
Patient breathing enough, but pt hypoxemic / hypercapneic
Patient breathing with normal gas exchange, but working hard
Airway protection
7. Indications
LABORATORY CRITERIA
CLINICAL CRITERIA
OTHER CRITERIA
8. LABORATORY CRITERIA Blood gases : PaO2 < 55 mm Hg
PaCo2 > 50 mm Hg
pH < 7.32
PFT : Vital Capacity < 10 ml/Kg
-ve inspiratory force <25cm H20
FEV 1 < 10 mL/Kg
9. Clinical criteria Apnea / Hypopnea
Respiratory distress with altered mentation
Clinically apparent increasing work of breathing unrelieved by other interventions
Need for airway protection
10. Other criteria
Controlled hyperventilation ( eg head injury )
Severe circulatory shock
THERE IS NO ABSOLUTE CONTRAINDICATION FOR MECHANICAL VENTILATION
11. Connections
12. connections
13. Connections
14. Self test To check : - leak
- compliance
- resistance of circuit
- sensors
Needs to be done :
- before connecting to patient
- once in 2 weeks
- whenever circuit is changed
15. Select mode
Depends on : Patients requirement
User comfort
Availability
16. Basic principles
For PO2 : adjust FiO2, PEEP
For PCo2 : adjust TV , RR
17. Set variables
18. MODE OF VENTILATION
Tailored to need of the patient
SIMV / A/C � versatile modes for initial settings
In pts with good resp drive & mild � mod resp failure � PSV
19. Tidal volume Initial TV : 5 � 8 ml/Kg of ideal bd wt
Lowest values are recommended in presence of Obstructive airway ds & ARDS
Goal : to adjust TV so that plateau pressures are less than 35 cm H20
20. Respiratory rate 8 � 12 breaths per minute : pts not requiring hyperventilation for treatment of toxic/metabolic acidosis or intracranial injury
Initial rate may be low ( 5 � 6 breaths per min ) in asthmatic pts where permissive hypercapnic technique is used
21. Supplemental o2 therapy
Lowest FiO2 that produces an
Sp02 > 90 %
PaO2 > 60 mm Hg
is recommended
22. Inspiration : expiration ratio
Normal I:E ratio to start is 1:2
Reduced to 1:4 or 1:5 in presence of obstructive airway disease in order to air trapping
Inverse I:E � in ARDS
23. INSPIRATORY FLOW RATE
60 L/min is typically used
Increased to 100 L/min : to deliver TVs quickly and allow for prolonged expiration in presence of obstructive airway ds
24. Positive end expiratory pressure ( peep ) Titrated according to PEEP and BP
High PEEP ( > 10 H20 ) � pneumonia, ards
PEEP � reduces risk of atelectasis
- increase no of open alveoli
( decrease V/Q mismatch )
- in CHF : decrease venous return
Physiological PEEP ( 3-5 cm H20 ) : to prevent decrease in FRC in normal lungs
25. Sensitivity ( TRIGGER )
Set at -1 to -2 cm H20
NEWER VENTILATORS SENSE INSPIRATORY FLOW
and thereby reduce work of breathing associated with ventilator triggering
26. SET VARIABLES Mode : Complete / Partial . VCV/PCV
Rate : titrate to Pco2
Tidal Volume : 5 � 8 ml / Kg
Flow rate & Pattern : 4 � 8 times Minute Ventilation
I:E = 1:2 to 1:4
FiO2 : titrate to O2 Saturation / Pa O2
PEEP : titrate to PaO2 & BP
Trigger : Adjust to synchronize
27. Alarm settings Fixed alarms : disconnection
o2 sensor
Set alarms : volume
pressure
rate
apnea
28. Monitor & reassess Patient
Monitor : pulse , bp , rr, spO2
Ventilator
Abg
Volume
Pressure
Rate
Patient comfort / synchrony
29. Ventilatory settings in various diseases
30.
For Paralysed pts : CMV or A/C mode
For Non paralysed pts : SIMV mode
Pts with normal resp effort
mild resp failure : PSV mode
31. Asthma & copd
Hypoxia corrected by High FiO2
Increase Expiratory Flow Time to max : to prevent increase intrinsicPEEP
RR : 6 -8 breaths / min ( permissive hypercapnia )
I : E : increased 1:2
32. ards A/C mode
Tidal Volume : 6 ml/Kg
PEEP : 5
Ventilatory rate : 12
titrated to maintain Ph > 7.25
33. Chf Respond well to positive pressure ventilation (opens alveoli, reduces preload)
Many benefit from trial of noninvasive CPAP / BiPAP
Intubated pts usually manage to oxygenate well
But PEEP can be increased to improve oxygenation and reduce preload
34. Thank you