Download
1 / 39
400 likes | 418 Views
Collaborative centers in Germany are improving outcomes for CRC liver metastases patients. Explore neoadjuvant chemotherapy and surgical options. Learn about prognostic factors and the impact of different chemotherapy regimens. Discover recent studies and guidelines for effective treatment.

E N D
Preoperative/neoadjuvant treatment of CRC liver metastases Markus Moehler
>350 Certified Colon Cancer Centers .. but how good are they in reality ?
The collaboration makes the difference Surgery of liver metastases can achieve long-term DFS Even in Germany, >4000 patients are undertreated with CRC liver metastases 100 80 60 neoadjuvant Chemo + OP 40 Chemo 20 30% ! BSC 0 Moehler, Thomaidis et al. J Cancer Res Clin Oncol 2015
The collaboration makes the difference Surgery of liver metastases can achieve long-term DFS 100 80 60 neoadjuvant Chemo + OP 40 Chemo 20 30% ! BSC 0 Moehler, Thomaidis et al. J Cancer Res Clin Oncol 2015
The collaboration makes the difference Our metastatic CRC patients survive >4 years 100 80 60 neoadjuvant Chemo + OP 40 Chemo 20 30% ! BSC 0 Moehler, Thomaidis et al. J Cancer Res Clin Oncol 2015
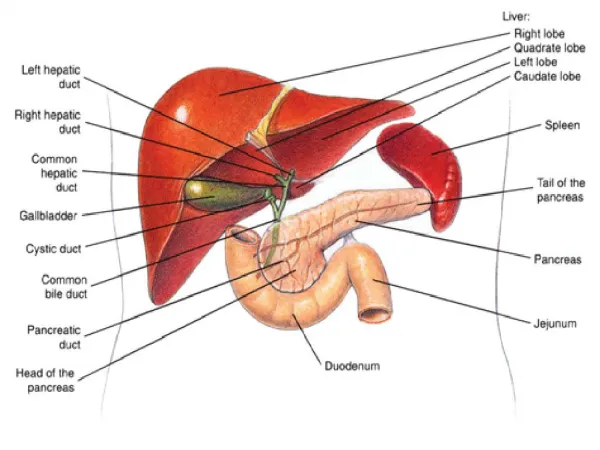
Mainz University Cancer Center Center of excellence for CRC liver metastases Firstcenter of excellence and competence General, Visceral & Transplant Surgery (AVTC
Mainz University Cancer Center Outreach / Regional Network To ensure the highest quality of cancer care for each patient at every place and any time
Mainz University Cancer Center Outreach / Regional Network Oncology Center (n=2) Hospital (n=12) Organ-specific Cancer Center (n=3) PracticingOncologist (n=22)
Mainz University Cancer Center Outreach / Regional Network UCT Network Communication • Virtual „centralentryportal“ • Password-protectedarea • Information oftrials, SOPs ... • Contactinformation at a glance • UCT hotline • Tumor Board participations • In personor via telecommunication • „Flying UCT oncologist“ Outreach / Regional Network
Colorectal cancer Resection ? Resection ? Resection ? Therapeutic Options in MetastaticDisease
Prognostic factors in CRC liver metastases Resection after neoadjuvant chemotherapy Technical Resectability Functionality of Remnant Liver tissue Involved Struktures/Segments
Prognostic factors in CRC liver metastases Technical Chemotherapy Technical Resectability Functionality of Remnant Liver tissue Involved Struktures/Segments
Prognostic factors in liver metastases Technical Chemotherapy • Number /size • Lymphnodestatus • Disease-freeInterval • CEA levels Technical Resectability Functionality of Remnant Liver tissue Involved Struktures/Segments
Prognostic factors in CRC liver metastases Technical Chemotherapy Conversion-chemotherapy(„neoadjuvant“) Technical Resectability • Techniques • presented by Dr. Tagkalos Morbidität Komplikationsrisiko Keine Resektionen
Prognostic factors in CRC liver metastases Response and Resection rates Studies with neoadjuvant focus Studies with met. CRC Jones, Folprecht Eur J Cancer 2014
Chemo+EGFR vs. Chemo +VEGFRAS wt RAS mutated RASWildtype Chemotherapy with biologicals is better Anti-VEGF Anti-EGFR
Chemo+EGFR vs. Chemo +VEGFRAS wt n RR PFS OS • FOLFIRI/Cetux17165%10.433.1 • FOLFIRI/Beva17160%10.2 25.6 • Heinemann, Lancet Oncol 2014 HR0.93HR 0.70 p=0.017
Chemo+EGFR vs. Chemo +VEGFRAS wt n RR PFS OS • FOLFIRI/Cetux17165%10.433.1 • FOLFIRI/Beva17160%10.2 25.6 • Heinemann, Lancet Oncol 2014HR0.93HR 0.70 p=0.017 • FOLFOX/Pani8864%13.041.3 • FOLFOX/Beva8261%9.528.9 • Schwartzberg, JCO 2014HR 0.65HR 0.63 p=0.058
Chemo+EGFR vs. Chemo +VEGFRAS wt n RR PFS OS • FOLFIRI/Cetux17165%10.433.1 • FOLFIRI/Beva17160%10.2 25.6 • Heinemann, Lancet Oncol 2014HR0.93HR 0.70 p=0.017 • FOLFOX/Pani8864%13.041.3 • FOLFOX/Beva8261%9.528.9 • Schwartzberg, JCO 2014HR 0.65HR 0.63 p=0.058 • Chemo/Cetux27069%11.432.0 • Chemo/Beva25654%11.331.2 • Lenz, ESMO 2014p<0.01 HR 1.1HR 0.9
Chemo+EGFR vs. Chemo +VEGFRAS wt n RR PFS OS • FOLFIRI/Cetux295 62%10.028.7 • FOLFIRI/Beva297 58% 10.3 25.0 • Heinemann, Lancet Oncol 2014p=0.18HR1.06HR 0.77 p=0.017 • FOLFOX/Pani142 58%10.9 34.2 • FOLFOX/Beva14354% 10.1 24.3 • Schwartzberg, JCO 2014 HR 0.84 HR 0.62 p=0.009 • Chemo/Cetux57866%resected: 82 pts (14.2%) • Chemo/Beva55957%resected: 50 pts (8.9%) • Venook, ASCO/WCGIC/ESMO 2014p<0.02p<0.01
FOLFOXIRI combinations n RR PFS OS FOLFOXIRI/Bev25265% 12.131.0 FOLFIRI/Bev 256 53% 9.7 25.8 Loupakis, NEJM 2014p<0.01 HR0.75 p<0.01 HR 0.79,p=0.054 Progression free survival Overall survival
Background: Resectability is often missed • Retrospective reviews suggest that careful patient selection is still a major challenge • CELIM (Chemo+Cetux) and Prodige-14 (Chemo + Cetux/Beva) report potential/real secondary resections of 50% and higher in LLD • The reported metastatic resection rate in FIRE-3 was 13% in ITT. • The new ESMO consensus guideline does not limit surgery and/or ablations to single-organ metastatic disease. • Therefore investigation of a mixed cohort appears important. Ychou M. et al. Prodige1$/ACCORD 21 (METHEP-2), J Clin Oncol 34, 2016 (suppl; abstr 3512). Folprecht G et al. Lancet Oncol 2010
Background (CELIM) - Improving resectability in mCRC- • Untreated mCRC • 32% • +28% • After combination- therapy • 60% Folprecht G, et al. Lancet Oncol 2010
Background FIRE-3 (all comers!) 1.0 0.75 0.50 Probability of survival 0.25 Δ = 8.1 months 0.0 48 12 60 36 24 72 months since start of treatment * KRAS and NRAS exon 2, 3 and 4 wild-type Stintzing S, …Moehler M, et al. Lancet Oncol. 2016
Review-Process • 448 patients, central, blinded for treatment and other reviewers • Baseline vs best response images were evaluated in pairs • Information given to reviewers during assessment: • metachronous (incl. disease-free interval) vs. synchronous • disease spread (as noted in CRF) • primary in place • 8 surgeons, 3 medical oncologists • Definition of resectability: ≥50% votes for resectability
FIRE-3, Assessment of resectability Lethal tumor load Baseline • DpR Tumor Nadir Definition of resectability: ≥50% votes for resectability 8 surgeons, 3 medical oncologists Time 448 patients, central, blinded for treatment and other reviewers
FIRE-3, Resectability at baseline Intention 100% 50% 50% 100% 21.7% Median kappa‘ coefficientfor inter-rater reliability: 0.56
FIRE-3, Resectability at best response 100% Intention 50% 50% 100% 53.1% Median kappa‘ coefficient for inter-rater reliability: 0.66
Resectability according to organ-involvement Evaluation at „baseline“ Evaluation at „best response“ Metastatic spread [CRF] N=186 One-organ disease N=186 Two-organ disease N=155 N=155 Three-organ disease N=80 N=80 Percentage with resectable disease Percentage with unresectable disease
Review (best response) vs. study-reports
Impact of treatment-site Percentage Difference in resection rate university vs. others: P=0.02 (Fisher‘s exact test)
The center makes the difference: Mainz UCT Survival CTX + anti-EGFR vs CTX + anti-VEGF: 47 vs 20 months Möhler, Thomaidis et al. J Cancer Res Clin Oncol (2015)
The collaboration makes the difference Our metastatic CRC patients survive >4 years 100 80 60 neoadjuvant Chemo + OP 40 Chemo 20 30% ! BSC 0 Moehler, Thomaidis et al. J Cancer Res Clin Oncol 2015
The collaboration makes the difference Our metastatic CRC patients survive >4 years LIMITATIONS in daily practice • Co-morbidities (in ECOG 0/1 pts) • Unclaritieswith lesions ( lymph nodes and lung) • Suspected vs. proven peritoneal lesions (Information not always exactly available) • Patient’s wish • Available liver-specific MRI/PET-CT scans may have changed some recommendations Moehler, Thomaidis et al. J Cancer Res Clin Oncol 2015
We all make the difference ! • Resectability can be increased from 22% at baseline to 53% at best response • CTX improves resectability even in patients with >1-organ disease. • Potential resections were evaluated as “easier” and the potential clinical benefit as “greater” at best response. • Resection-rates will be highest in university-hospitals and lowest in private practice: collaboration necessary ! • Regular and pre-planned assessment of mCRC-patients with specialized surgeons in high-volume institutions may help to increase resection rates.
We all make the difference ! Expandingbounderiesforourpatients • New moleculardiagnostics (NGS, Liquid biopsies) • Multidisciplinaryteamswith high clinicalimpact • Frompalliative therapyinto potential cure • From non-resectableintoresectabletumors • Immunotherapyforadjuvantandadvancedindications
Thank you very much for all your commitment and enthusiasm !!