Download
1 / 1
10 likes | 106 Views
Diabetes Prevention: Targeting Preconceptional Women Danielle Symons Downs, Ph.D., Carol S. Weisman, Ph.D., Marianne Hillemeier, Ph.D., and John J. Botti, M.D. Departments of Kinesiology, Health Evaluation Sciences, Health Policy and Administration, and Obstetrics and Gynecology.

E N D
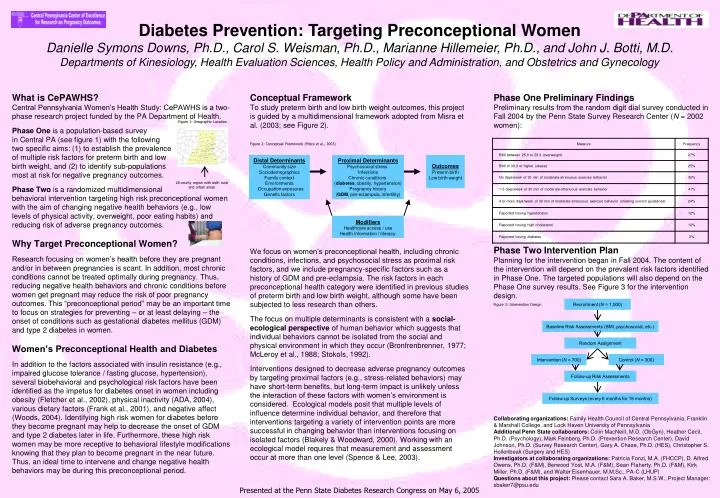
Diabetes Prevention: Targeting Preconceptional Women Danielle Symons Downs, Ph.D., Carol S. Weisman, Ph.D., Marianne Hillemeier, Ph.D., and John J. Botti, M.D. Departments of Kinesiology, Health Evaluation Sciences, Health Policy and Administration, and Obstetrics and Gynecology What is CePAWHS? Central Pennsylvania Women’s Health Study: CePAWHS is a two-phase research project funded by the PA Department of Health. Phase One is a population-based survey in Central PA (see figure 1) with the following two specific aims: (1) to establish the prevalence of multiple risk factors for preterm birth and low birth weight, and (2) to identify sub-populations most at risk for negative pregnancy outcomes. Phase Two is a randomized multidimensional behavioral intervention targeting high risk preconceptional women with the aim of changing negative health behaviors (e.g., low levels of physical activity, overweight, poor eating habits) and reducing risk of adverse pregnancy outcomes. Why Target Preconceptional Women? Research focusing on women’s health before they are pregnant and/or in between pregnancies is scant. In addition, most chronic conditions cannot be treated optimally during pregnancy. Thus, reducing negative health behaviors and chronic conditions before women get pregnant may reduce the risk of poor pregnancy outcomes. This “preconceptional period” may be an important time to focus on strategies for preventing – or at least delaying – the onset of conditions such as gestational diabetes mellitus (GDM) and type 2 diabetes in women. Women’s Preconceptional Health and Diabetes In addition to the factors associated with insulin resistance (e.g., impaired glucose tolerance / fasting glucose, hypertension), several biobehavioral and psychological risk factors have been identified as the impetus for diabetes onset in women including obesity (Fletcher et al., 2002), physical inactivity (ADA, 2004), various dietary factors (Frank et al., 2001), and negative affect (Woods, 2004). Identifying high risk women for diabetes before they become pregnant may help to decrease the onset of GDM and type 2 diabetes later in life. Furthermore, these high risk women may be more receptive to behavioral lifestyle modifications knowing that they plan to become pregnant in the near future. Thus, an ideal time to intervene and change negative health behaviors may be during this preconceptional period. Conceptual Framework To study preterm birth and low birth weight outcomes, this project is guided by a multidimensional framework adopted from Misra et al. (2003; see Figure 2). We focus on women’s preconceptional health, including chronic conditions, infections, and psychosocial stress as proximal risk factors, and we include pregnancy-specific factors such as a history of GDM and pre-eclampsia. The risk factors in each preconceptional health category were identified in previous studies of preterm birth and low birth weight, although some have been subjected to less research than others. The focus on multiple determinants is consistent with a social-ecological perspective of human behavior which suggests that individual behaviors cannot be isolated from the social and physical environment in which they occur (Bronfrenbrenner, 1977; McLeroy et al., 1988; Stokols, 1992). Interventions designed to decrease adverse pregnancy outcomes by targeting proximal factors (e.g., stress-related behaviors) may have short-term benefits, but long-term impact is unlikely unless the interaction of these factors with women’s environment is considered. Ecological models posit that multiple levels of influence determine individual behavior, and therefore that interventions targeting a variety of intervention points are more successful in changing behavior than interventions focusing on isolated factors (Blakely & Woodward, 2000). Working with an ecological model requires that measurement and assessment occur at more than one level (Spence & Lee, 2003). Phase One Preliminary Findings Preliminary results from the random digit dial survey conducted in Fall 2004 by the Penn State Survey Research Center (N = 2002 women): Phase Two Intervention Plan Planning for the intervention began in Fall 2004. The content of the intervention will depend on the prevalent risk factors identified in Phase One. The targeted populations will also depend on the Phase One survey results. See Figure 3 for the intervention design. Collaborating organizations: Family Health Council of Central Pennsylvania, Franklin & Marshall College, and Lock Haven University of Pennsylvania Additional Penn State collaborators: Colin MacNeill, M.D. (ObGyn), Heather Cecil, Ph.D. (Psychology), Mark Feinberg, Ph.D. (Prevention Research Center), David Johnson, Ph.D. (Survey Research Center), Gary A. Chase, Ph.D. (HES), Christopher S. Hollenbeak (Surgery and HES) Investigators at collaborating organizations: Patricia Fonzi, M.A. (FHCCP), D. Alfred Owens, Ph.D. (F&M), Berwood Yost, M.A. (F&M), Sean Flaherty, Ph.D. (F&M), Kirk Miller, Ph.D. (F&M), and Walter Eisenhauer, M.M.Sc., PA-C (LHUP) Questions about this project: Please contact Sara A. Baker, M.S.W., Project Manager: sbaker7@psu.edu Figure 1: Geographic Location Figure 2: Conceptual Framework (Misra et al., 2003) Distal Determinants Community size Sociodemographics Family context Environments Occupation exposures Genetic factors Proximal Determinants Psychosocial stress Infections Chronic conditions (diabetes, obesity, hypertension) Pregnancy history (GDM, pre-eclampsia, infertility) Outcomes Preterm birth Low birth weight 28 county region with both rural and urban areas Modifiers Healthcare access / use Health information / literacy Figure 3: Intervention Design Recruitment (N = 1,000) Baseline Risk Assessments (BMI, psychosocial, etc.) Random Assignment Intervention (N = 700) Control (N = 300) Follow-up Risk Assessments Follow-up Surveys (every 6 months for 18 months) Presented at the Penn State Diabetes Research Congress on May 6, 2005