Download
1 / 39
430 likes | 663 Views
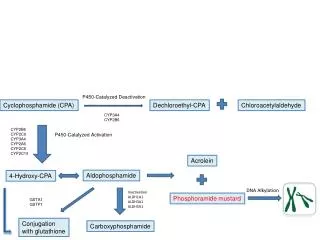
Cyclophosphamide vs Mycophenylate mofetil for lupus nephritis. The curse of living in interesting times?. Mary Anne Dooley March, 2009. Cytotoxic Therapy Prolongs Renal Survival. Improved RENAL not overall survival All classes of renal histology included 100% Caucasian

E N D
Cyclophosphamide vs Mycophenylate mofetil for lupus nephritis The curse of living in interesting times? Mary Anne Dooley March, 2009
Improved RENAL not overall survival All classes of renal histology included 100% Caucasian Long duration (11 months) of nephritis prior to entry Excluded patients with renal insufficiency Quarterly cyclophosphamide therapy employed Comorbidities over time not reported The “NIH Protocol”
Racial Disparity: Renal Survival for Class IV Lupus Nephritis Treated with IV CTX N=39 N=51 % Probability of renal survival p=0.007 Years from renal biopsy M Dooley et al, Kidney Int 1997; 51:1188-1195
Renal Survival by Race at UNC Independent of the following factors: • Age • Duration of SLE • History of hypertension • Hypertension control during therapy • Activity or chronicity indices on renal biopsy • Pattern of corticosteroid therapy
Diffuse GN (WHO IV) Majority African American cohorts Majority caucasian cohorts Austin, Sem Nephrol 19:2, 1999
Racial Disparity in response to cyclophosphamide Boumpas, Lancet 340:741, 1992
Relapse Proportion withoutrelapse Time (mo from starting IV CYC) Re-remission Median time 32 mo Median time 79 mo 20% relapse after 18 mo Time (mo from starting IV CYC) Remission, relapse, and re-remission of proliferative lupus nephritis treated with cyclophosphamide Remission Median time 10 mo 22% failed to remit after 2 yr Proportion withoutremission Time (mo from starting IV CYC) Proportion withoutre-remission Ioannidis JA et al. Kidney Int 2000; 57:258-264.
Remission rates: MMF vs IVC Intent-to-Treat analysis p = 0.009 37/71 p = NS p = 0.005 Responding (%) 21/69 21/71 17/69 16/71 4/69
MMF 6 early 5 severe disease 1 non-compliance 3 late 2 crossover refusals 1 toxicity (rash) No deaths IVC 13 early 3 treatment refusals (1 death) 3 severe disease (2 deaths) 6 non-compliance (2 with GI toxicity) 1 lymphopenia 2 late 2 lost to follow-up Study withdrawals
University of Miami Study Methods: Study design & patient population • Open label, randomized clinical trial • Inclusion criteria • Adults > 18 years of age, World Health Organization (WHO) classes III, IV, V with proliferation • Exclusion criteria • Have received IVCY > 7 doses or AZA > 8 weeks • Creatinine clearance < 20 mL/min • Pregnancy • Any clinically significant infection within 2 weeksof enrollment
Patient survival 1.00 0.75 Cumulative probability 0.50 p = 0.11, MMF vs IVCY p = 0.02, AZA vs IVCY p = 0.33, MMF vs AZA 0.25 19 19 15 10 9 4 2 AZA 20 19 12 6 3 2 1 IVCY 20 20 14 11 6 2 2 MMF 0.00 72 0 12 24 36 48 60 Time (months)
Free of relapse p = 0.021, MMF vs IVCY p = 0.124, AZA vs IVCY p = 0.222, MMF vs AZA 1.00 0.75 0.50 Cumulative probability 0.25 19 15 10 6 4 3 1 AZA 17 10 4 2 2 1 1 IVCY 19 17 12 8 3 2 1 MMF 0.00 0 12 24 36 48 60 72 Time (months)
MMF vs. CTX for Lupus Nephritis 350 Patient Two-Phase study with a 6 month induction followed by up to 3 year maintenance
Euro-Lupus Nephritis Trial Houssiau FA. Arthritis Rheum 50:3934-3940
Excluded (n = 90) Assessed (n = 460) Randomized (n = 370) Open-label treatment MMF IVC Allocated to MMF (n = 185) Received MMF (n = 184) Withdrawals (n = 35) Due to adverse event (n = 24) Consent withdrawn (n = 6) Other reason (n = 5) Allocated to IVC (n = 185) Received IVC (n = 180) Withdrawals (n = 29) Due to adverse event (n = 13) Consent withdrawn (n = 5) Other reason (n = 11) Primaryendpoint: responders in randomized population (n = 370) Responders Maintenance phase Double-blind re-randomization to corticosteroids plus MMF or azathioprine for up to 3 years
Treatment Compliance Oral corticosteroids twice daily
Primary Endpoint: Responders at Month 6 • Response was judged by a blinded Clinical Endpoint Committee, by the criteria: • Decrease in urine protein/creatinine ratio (P/CR) • – to <3 in patients nephrotic at baseline (P/CR ≥3), • – or by ≥50% in patients subnephrotic at baseline (P/CR <3) • and • Stabilization of serum creatinine level (24-week level ±25% of baseline), or improvement MMF IVC MMF was not superior to IVC(p = 0.575)
Key Renal Secondary Endpoints • Complete remission as defined by: • return to normal serum creatinine level • proteinuria ≤500 mg/24 hr • inactive urinary sediment • Remission in each one of these individual parameters • Anti-dsDNA, C3, C4 and serum albumin
Remission Rates by Renal Criteria No significant differences between groups in complete remission or by individual criteria
Summary of Deaths • MMF group: 2 deaths in Argentina, 6 in China, and 1 in Malaysia • IVC group: 2 deaths in the USA, 2 in China, and 1 in the UK • MMF group: 7 deaths were due to infections and none due to SLE • IVC group: 2 deaths due to infections, 2 due to SLE
Summary Study did not meet its primary objective of showing that MMF was superior to IVC Response rates with MMF were consistent across racial, ethnic, and regional groups Response rates lower with IVC compared with MMF in non-Caucasian, non-Asian patients, ethnically Hispanic patients, and patients in Latin America AE profiles for MMF and IVC were broadly similar over 24 weeks, and consistent with previous reports Overall incidence of adverse events and infections similar between racial groups Ongoing maintenance phase compares MMF with azathioprine for up to 3 years
Degree and durability of remission not optimal for many patients • Many patients fail to achieve complete remission • Less than 50% survival without end-stage renal disease (ESRD) at 10 years in absence of complete remission. • Significant rates of renal flare despite maintenance therapy • Adverse events can limit effective dosing of common maintenance therapies for lupus nephritis • High cost burden associated with lupus nephritis • Costs escalate with degree of renal damage
Many Patients Do Not Achieve Complete Remission Following Induction Prevalence of Complete Remission in Lupus Nephritis Following Induction Therapy (24 weeks) Percentage of Patients N = 140 (Intent-to-treat analysis) Complete remission defined as return to within 10% of normal values of serum creatinine, proteinuria, and urine sediment. Source: Ginzler et al. NEJM. 2005; 353(21)
Importance of Maintaining Complete Remission in Lupus Nephritis Results of a long-term prospective study in patients with diffuse lupus nephritis Patient Survival Without ESRD at 10 Years Patient survival without ESRD less than 50% at 10 years with partial remission Percentage of Patients Surviving Without ESRD P<0.0001 (CR vs PR) N = 86 Partial Remission: 50% reduction in baseline proteinuria to < 1.5 g/d with not more than 25% increase in baseline sCr. Complete Remission: Proteinuria < 0.33 g/d and serum creatinine < 1.4 mg/dl Source: Chen et al. Clin J Am Soc Neph. 2008; 3(1)
Common Maintenance Therapies for Lupus Nephritis Often Do Not Prevent Renal Flare * Maintenance therapy given at physician discretion; 75% of patients received AZA maintenance therapy.