Download
1 / 27
280 likes | 574 Views
ROLE OF RENAL BIOPSY IN SILENT LUPUS NEPHRITIS. M.E. Guerra 1 , Y. Arce 2 , M.M Díaz 3 , P. Moya 4 . J. Ballarín 3 , F. Algaba 5 1 Department of Pathology . Central University Hospital of Asturias, Oviedo. Spain 2 Department of Pathology . Puigvert Foundation , Barcelona. Spain .

E N D
ROLE OF RENAL BIOPSY IN SILENT LUPUS NEPHRITIS M.E. Guerra1 , Y. Arce2, M.M Díaz3, P. Moya4. J. Ballarín3, F. Algaba5 1Department of Pathology. Central University Hospital of Asturias, Oviedo. Spain 2Department of Pathology. PuigvertFoundation, Barcelona. Spain. 3Department of Nephrology. PuigvertFoundation, Barcelona. Spain 4Department of Rheumatology. Sant Pau Hospital, Barcelona. Spain. 5Department of Pathology. PuigvertFoundation, Barcelona. Spain.
INTRODUCTION • SystemicLupus Erythematosus(SLE) is a multisystemautoimmunediseaseprimarilyaffectingwomen of reproductiveage. • Kidneydiseasedevelops up to 60% of patientswith SLE: • 15-20% firstclinicalmanifestation. • 25-50% had renal involvement at the time of lupus diagnosis. • Important cause of morbility, evenmortality. • Goalsformanagingpatientswith lupus nephritis (LN): • Earlydiagnosis • Properand prompttherapytoprevent irreversible damagewithoutexposure of sideeffects of immunosupressors.
INTRODUCTION • Renal Biopsyisessentialtodiagnosespecificform of LN: • Biologicalmarkers (serumlevels C3, C4, anti-DNA): lowsensitivitytopredictactivitydisease and risktodevelop new flares. • Discrepanciesbetweenclinicalpresentation and pathologicfindings. • LN isnot a staticentity. • Impliesdifferent prognosis and therapeuticapproaches. • Repeat biopsy in LN flares is a matter of controversy. • Its role is still not defined after clinical remission. • Daleboudt Gabrielle M. N. et al. Nephrol Dial Transplant (2009) • Hsieh YP. ClinNephrol 2012; 77: 18-24.. • Seshan S. Arch Pathol Lab Med. 2009;133:233–48.
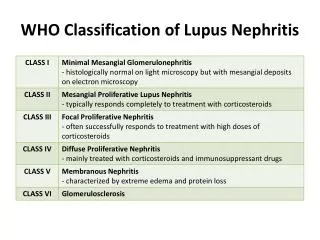
SILENT LUPUS NEPHRITIS (SLN) • Moroni G. Am J Kidney Diseases.1999; 34:530–9. • Yoo CW. Nephrol Dial Transplant. 2000;15:1604–8. • Cavallo T. Am J Pathol1977;87:1–13 • Ahmadian YS, Am J Dis Child 1972;123: 121 – 125. • Zabaleta-Lanz M et al. Lupus 2003;12:26-30. • Zabaleta-Lanz M et al. Inmunol 2004; 23: 278-83. • Zabaleta-Lanz M et al. Lupus 2006; 15: 845-51.
OBJECTIVES • Evaluatefrequency of SLN in patientswith at leastoneprevious renal flarewithhistologicalconfirmation, afterinduction/maintenancetreatment, thatachieved complete renal and clinicalremission. • Correlate complete renal remissionwithhistologicalfindings and compare themtothoseobseved in previousbiopsy. • Examine theinfluence of histologicalchange in thetherapeuthicdecision.
MATERIAL AND METHODS • Prospectiveand descriptivestudy. • Review of patientsdiagnosed of SLE , as definedby American RheumatismAssociation, thathad LN biopsy-proven. • Selection of patientswhofulfillcomplete remission (CR) criteriafor at least 2 years. 2nd biopsyisperformed at thismoment CR criteria: • Proteinuria < 50mg/mmolcreatinine. • Normal renal function. • Inactive urinesediment. • Biopsieswerecategorizedaccordingto ISN/RPS classificationprotocol. • Activityand chronicityindexweredeterminedaccordingtothescoringsystem of Pollack et al., as modifiedby Austin et al. • WeeningJJ et al. J Am SocNephrol2004; 15:241-250. • Weening JJ et al. KidneyInt 65 2004;15: 521-530.
MATERIAL AND METHODS • Prospectiveand descriptivestudy. • Review of patientsdiagnosed of SLE , as definedby American RheumatismAssociation, thathad LN biopsy-proven. • Selection of patientswhofulfillcomplete remission (CR) criteriafor at least 2 years. 2nd biopsyisperformed at thismoment CR criteria: • Proteinuria < 50mg/mmolcreatinine • Normal renal function. • Inactive urinesediment. • Biopsieswerecategorizedaccordingto ISN/RPS classificationprotocol. • Activityand chronicityindexweredeterminedaccordingtothescoringsystem of Pollack et al., as modifiedby Austin et al. • WeeningJJ et al. J Am SocNephrol2004; 15:241-250. • Weening JJ et al. KidneyInt 65 2004;15: 521-530.
ACTIVITY AND CHRONICITY INDICES (NIH) ActivityIndex(0-24): - Endocapillaryhypercellularity (0-3+) - Leucocyteinfiltration (0-3+) - Subendothelialhyalinedeposits (0-3+) - Fibrinoidnecrosis / karyorrhexis: (0-3+) x 2 - Cellularcrescents (0-3+) x 2 - Intersticial inflammation (0-3+) ChronicityIndex(0-12): - Glomerular sclerosis (0-3+) - Fibrouscrescents (0-3+) - Tubular atrophy (0-3+) - Intersticial fibrosis (0-3+) 0: Absent 1+: <25 % glomeruliaffected 2+: 25-50 % glomeruliaffected 3+: > 50 % glomeruliaffected • Austin HA 3rd, Muenz LR, Joyce KM, Antonovych TA, Kullick ME, Klippel JH, Decker JL, Balow JE Kullick ME.. .Am J Med 1983 Sep;75(3):382-91. • Austin HA 3rd, Muenz LR, Joyce KM, Antonovych TT, Balow JE. Kidney Int.1984 Apr;25(4):689-95
MATERIAL AND METHODS • Collecting data • Demographic • Clinical (SLEDAI) • Analitical • Renal histology: • International Society of Nephrology/Renal PathologySocietyClassification of Lupus Nephritis 2004 (ISN/RPS). • Activity and ChronicityIndex.
RESULTS RENAL BIOPSY PRE-COMPLETE REMISSION
RESULTS RENAL BIOPSY AFTER COMPLETE REMISSION
RESULTS V IV III II 100% patientswith SLN
HISTOLOGICAL IMPROVEMENT 70% Biopsy Pre-CR Class III or IV Biopsyafter CR Class II o
NO HISTOLOGICAL CHANGE 30% Biopsyafter CR Class II+V Biopsy Pre-CR Class II+V
RESULTS CI AI AI(CR) CI(CR) ActivityIndexdecreases
CONCLUSION • No patients achieve complete histological remission. • Membranous pattern and mesangial proliferation remains, meanwhile endocapillary proliferation dissapears. • Activity Index decreases and Chronicity Index remains the same. • Renal biopsy in Complete Remission implicates a change in therapeutic decision in 50% of cases in our series. Silent Lupus Nephritisishighlyprevalent in patientswithSystemic Lupus Erythematosus, being renal biopsythegoldstandardforits diagnosis.