Download
1 / 37
370 likes | 612 Views
Cardiomyopathies. By:Dawit Ayele ( MD,Internist ). Definition. a group of diseases that affect the heart muscle itself and are not the result of hypertension , congenital, valvular , coronary, or pericardial abnormalities. Classification.

E N D
Cardiomyopathies By:DawitAyele (MD,Internist)
Definition • a group of diseases that affect the heart muscle itself and are not the result of hypertension , congenital, valvular, coronary, or pericardial abnormalities
Classification • based on LV cavity size, wall thickness, and systolic contraction • dilated (myocyte necrosis, profound dilation, and systolic dysfunction), • hypertrophic(disproportionate septal thickening, obstructive or non-obstructive), or • restrictive (generalized wall thickening with both systolic and diastolic impairment)
Dilated Cardiomyopathy • Is mainly due to Prolonged, uninterrupted biomechanical overload • is characterized by eccentric hypertrophy(dilatation) , loss of cardiac contractile function(hypokinesis), and loss of cardiomyocytes due to apoptosis.
Epidemiology • Prevalence is increasing • About 1 in 3 cases of CHF in the west is due to dilated cardiomyopathy • More common in middle aged men & African Americans than whites
Causes • Idiopathic • Familial/genetic- 20-40% mostly autosomal dominant transmission • infection, (viral esp) • inflammation, • Toxins-(alcohol,cocain) • Pregnancy • Thyroid disease • Chronic uncontrolled tachycardia • collagen vascular disease, and • musculoskeletal disease
Clinical Manifestations • Of left & right sided CHF • Some present with left ventricular dilatation for months to yrs before diagnosis • Vague chest pain-but typical angina is unusual • Syncope 20 to arrhythmia or systemic embolism
Physical Examination • Variable degrees of cardiac enlargement • Advanced disease-narrow pulse pressure -Raised JVP -S3 & S4 sounds common -Mitral & tricuspid regurgitation may occur
Lab examinations • CXR-enlargement of cardiac silhoutte -may show evidence of pulmonary venous hypertension -may show interstitial & alveolar edema • ECG- • *Echocardiography • Cardiac catheterization • Coronary angiography • Transvenousendomyocardial biopsy-usu.not necessary
Treatment • Majority esp >55 yrs die within 3 yrs of onset of sxs • Target: - Avoid toxins including alcohol -Control CHF-standard Management -Chronic anticoagulation –prevent embolism -Sometimes pacemaker & use of implantable cardioverterdefibrillator -cardiac transplantation for refractory cases
HYPERTROPHYIC CARDIOMYOPATY is a genetic disorder characterized by disproportionate hypertrophy of the left ventricle, and occasionally of the right ventricle
Epidemiology • Prevalence • 1:500[0.2%] in general population(may be the most common genetically transmitted cardiac disorder) • 0.5% in non-selected Echo referral • Most common cause of Sudden cardiac death in the young in the USA • Usually in third or fourth decades
Etiology - Genetic: Familial HCM-Autosomal dominant(50%) Sporadic due to spontaneous mutations - Idiopathic
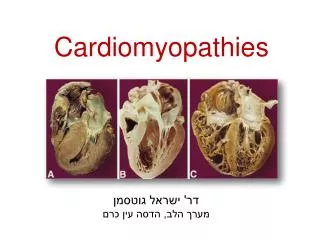
Pathology(Gross) -marked in myocardial mass -more LV involvement in hypertrophy -small ventricular cavities -dilated atria & hypertrophy (vent. filling resistance ) - MV& elongation -anomalous papilaryms. insertion.
Pathology(Gross) -variable pattern & extent of hypertrophy (Maj.IVS and anterolateral free wall) -Eventual burned-out phase in 5-10% of patient • Resemble DCM • Thinning, dilation, systolic dysfunction -Clinically silent remodeling with subtle regression of hypertrophy in some patient
Pathology (microscopic) -Myocardial hypertrophy -Gross disorganization of muscle bundles(whorled pattern) -Cell to cell arrangement abnormality(disarray) -Prominent fibrosis -interstitial connective tissue elements. -Abnormal intramural coronary arteries(80%)
Clinical feature ---Symptoms • Asymptomatic in majority [90%] • Sudden death can be the 1st event [esp. during extreme exertion] • Variable pattern and severity of symptoms • Dyspnea most common [90%] • Angina [75%] • Fatigue, presyncope and syncope common [not ominous in adult] • Palpitation, PND and dizziness less common • Exacerbating factors • Exercise • Erect posture [graying out spells]
Physical Examination - Normal except for an S4 Asymptomatic without – pressure gradient • Mild hypertrophy • Apical hypertrophy - Usually prominent in presence of pressure gradient • Characteristic carotid pulse [“spike and dome”] • Prominent “a” wave • Displaced, diffuse and abnormally forceful AI
Physical exam… • Narrow or paradoxical S2 split • S3 may be present [no prognostic value unlike in valvular AS] • Occasionally systolic ejection click • Systolic murmurs…midsystolic and hollosystolic [associated MR] • Correlate with SAM and pressure gradient • Labile intensity and duration • *Influenced by maneuvers • Diastolic murmurs…..apical rumbling and high pitched AR
Investigation • 1-ECG • 2-CXR(N/cardiomegaly+/-calcification) • 3-Echocardiography • 4-Other imaging-radionuclide scan,cardiac MRI(when Echo is technically inadequate) • 5-Cardiac catheterization(CAD,invasive Rx) • 6-Biopsy • 7-Genetic analysis?
The subcostal view from the two dimensional echocardiogram shows extremely hypertrophied and asymmetric septum which is 35 mm in thickness.
Management Guiding principles:Threeimportant goals • Symptoms alleviation • Complication prevention • Death risk reduction Majority require only medical treatment At least 50% with sever symptoms improve Invasive modalities required in only 5-10% **Myotomy-myectomy[ gold standard..70-90%]
Management… Condition & medics that better be avoided - physical exertion&competitive sports - digitalis glycosides unless A-fib or systolic dysfunction -B-adrenergic agonist -Nifedipine -excessive use of diuretics & dehydration
Hallmark of Constrictive Pericarditis • Abnormal diastolic function • Excessively rigid ventricular walls that impede filling • Unimpaired systolic function *Has functional resemblance with constrictive pericarditis *Is the least common of the main 3 CMPs
Classification of types according to cause • Myocardial-Non Infiltrative:*Idiopathic CMP Familial Scleroderma -Infiltrative:*Amyloidosis *Sarcoidosis -Storage disease Hemochromatosis.. • Endomyocardial -*Endomyocardial fibrosis -*Radiation -*Toxic effects of anthracyclin -eosinophilic syndrome -metastatic cancers -Drugs(Serotonin,ergotamin,busulfan..)
Pathologic processes - Myocardial fibrosis - Infiltration - Endomyocardial scarring - Myocyte hypertrophy in idiopathic variety
General Clinical Features • Depends on which ventricle & AV valve show predominant involvement • Thromboembolic complication ~1/3 • Sx-Exercise intolerance & dyspnea are the most prominent sxs.(inability to CO by tachycardia w/o compromising vent filling) -Exertional chest pain -Dependent edema,ascites & enlarged tender & often pulsatileliverpersistentlyvenous pressure.
Physical Exam • Distended JVP-doesn’t fall normally - +/- kussmaul’s sign *apex pulse is usually palpable • Ht sounds may be distant • S3, S4 or both
Investigations • ECG • CXR to R/O ddx-eg-constrictive pericarditis • Echocardiography – • Cardiac catheterization– • Endomyocardial biopsy, computed tomography or magnetic resonance imaging & others help distinguish restrictive & constrictive disease
Treatment & prognosis • No specific therapy other than symptomatic is available for the idiopathic form of RCM • Few secondary forms may benefit from targeted treatment regimens: • Hemochromatosis: deferoxamine has been helpful in reducing myocardial iron content • Chronic anticoagulation is often recommended to reduce the risk of embolization from the heart. • The prognosis in RCM is variable: usually it is one of relentless symptomatic progression and high mortality.