Download
1 / 88
900 likes | 1.23k Views
Cardiomyopathies. Roger Kersten D.O., FACC. Cardiomyopathies. The cardiomyopathies are a diverse group of disease that are not related to the usual causes of heart disease such as hypertension, valvular, congenital or pericardial disease.

E N D
Cardiomyopathies Roger Kersten D.O., FACC
Cardiomyopathies • The cardiomyopathies are a diverse group of disease that are not related to the usual causes of heart disease such as hypertension, valvular, congenital or pericardial disease. • Cardiomyopathies are classified according to anatomic or hemodynamic characteristics and etiology.
CardiomyopathiesFunctional Classification • Dilatated (congestive, DCM, IDC) • ventricular enlargement and systolic dysfunction • Hypertrophic (IHSS, HCM, HOCM) • inappropriate myocardial hypertrophyin the absence of HTN or aortic stenosis • Restrictive (infiltrative or myocardial scarring) • abnormal filling and diastolic function
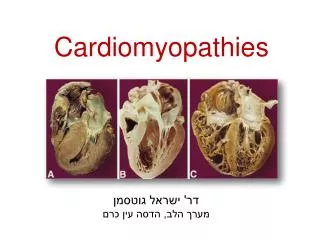
Morphologic and Hemodynamic Characteristics of the Cardiomyopathies Dilated Hypertrophic Restrictive Obliterative(Restrictive-Obliterative) Morphologic Biventricular dilatation Marked hypertrophy of leftventricle and occasionallyof right ventricle; usuallybut not always,disproportionatehypertrophy of septum Reduced ventricularcompliance; usuallycaused by infiltrationof myocardium (e.g., byamyloid, hemosiderin,or glycogen deposits) Thickened endocardiumor mural thrombi, or both,act as space-occupyinglesions Hemodynamic Cardiac output Normal Normal to Normal or Stroke volume Normal or ↑ Normal or Normal or Ventricular fillingpressure ↑↑ Normal or ↑ ↑↑ Usually ↑ Chamber size ↑↑ Normal or Normal or ↑ Typically Ejection fraction ↑↑ Normal to Normal to Diastolic compliance Normal or Other findings May have associatedfunctional mitral ortricuspid regurgitation Obstruction may developbetween interventricularseptum and septal leafletof mitral valveMitral regurgitation maybe present Characteristic ventricularpressure tracings thatresemble those recordedin constrictive pericarditis,with early diastolic dip-and-plateau configuration May be seen as a featureof the hypereosinophilicsyndromesSome investigators considerit a form of restrictivecardiomyopathy
Secondary Cardiomyopathies • When a cardiomyopathy has a definite etiology (e.g. sarcoidosis, infectious, scleroderma) – signs of that process are usually evident. • On rare occasions, cardiac involvement may precede other systemic manifestations.
Unknown cause(primary) Dilated Hypertrophic Restrictive Specific heart muscle disease (secondary) Infective Metabolic Systemic disease Heredofamilial Hypersensitivity Toxic Ischemic CardiomyopathiesWHO Classification Br Heart J 1980; 44:672-673
Etiologic Classification of Cardiomyopathies Cardiomyopathies of Unknown Etiology Idiopathic dilated cardiomyopathy –DCM Peripartum cardiomyopathy -DCM*Hypertrophic cardiomyopathy -HCMEndomyocardial fibrosis -RCMSubendocardial fibroelastosis -RCMEosinophilic endomyocardial disease -RCM (Löefflerendocarditis or fibroplastic endocarditis)Right ventricular dysplasia -DCMIdiopathic restrictive cardiomyopathy -RCM *may be reversible
Idiopathic Secondary Pregnancy Alcohol/Drugs Medications Tachycardia induced Sleep apnea? Infectious Ischemic Nutritional Obesity Dilated (Congestive) Cardiomyopathies
Etiologic Classification of Cardiomyopathies Dilated Cardiomyopathies of Known Etiology InfectiousViral and rickettsial myocarditis (e.g., HIV, Coxsackie B,* CMV*)Septic (bacterial endocarditis*)SyphilisParasitic disease (e.g., Chagas disease, trichinosis, toxoplasmosis)*Bacterial toxins (e.g., diphtheria toxin- associated with heart block) or hypersensitivity(rheumatic fever) *may be reversible
Etiologic Classification of Cardiomyopathies Dilated Cardiomyopathies of Known EtiologyToxic (partial list)Alcohol* (May take >10 years)Cobalt* (previously in beer)Carbon tetrachlorideCarbon monoxide*Thoridazine drugsAnticancer agents (e.g. daunorubicin doxorubicin, cyclophosphamide)Antimonials, Lead, MercuryCocaine*Antiretroviral agents (e.g., zidovudine,* dideoxyinosine*)Interferon alpha, IL2 *may be reversible
Etiologic Classification of Cardiomyopathies Dilated Cardiomyopathies of Known Etiology Systemic Diseases Neuromuscular syndromes:Muscular dystrophies (i.e. Duchene’s progressive muscular dystrophy, end stage Friedreich’s ataxia, Limb-Girdle dystrophy of Erb, Fascioscapularhumeral disease.)Collagen vascular disease (scleroderma) Diabetic (small vessel) Hemochromatosis Hurlers, Neiman-PicEndocrine diseases* (e.g., thyrotoxicosis, myxedema, pheochromocytoma, acromegaly, Cushings) * may be reversible
Etiologic Classification of Cardiomyopathies Dilated Cardiomyopathies of Known Etiology Nutritional Beriberi (thiamine deficiency)*Selenium deficiency*Kwashiorkor Hyophosphatemia*, Hypocalcemia* Carnitene deficiency* * Potentially reversible.
Etiologic Classification of Cardiomyopathies Cardiomyopathies of Known Etiology Ischemic * (hibernating myocardium) * Potentially reversible
Congestive (Dilated) Cardiomyopathy- Definition • A disease of unknown etiology that principally affects the myocardium. • LV dilatation and systolic dysfunction. • Pathology • increased heart size and weight. • ventricular dilatation, normal wall thickness. • heart dysfunction out of portion to fibrosis.
Secondary Congestive (Dilated) Cardiomyopathy • Infectious and Autoimmune processes (Myocarditis) • Coxsackie B etc. • Autoimmune processes • Acute Myocarditis vs. Congestive Cardiomyopathy • Fever with CHF • Pericarditis • Elevated CPK – MB , TnT ( less than 30% of myocarditis)
Dilated (Congestive) Cardiomyopathy • A familial form may be present in 10 – 30% • Characterized by diminished myocardial contractility • Reflected in reduction of systolic function. ( EF , LV EDP , SV , C.O ) • RV dysplasia characterized by RV failure and VT
Dilated (Congestive)CardiomyopathyClinical Manifestations • Highest incidence in middle age • blacks 2x more frequent than whites • men 3x more frequent than women • symptoms may be gradual in onset • acute presentation • misdiagnosed as viral URI in young adults • uncommon to find specific myocardial disease on endomyocardial biopsy
Dilated (Congestive) Cardiomyopathy • Clinical Features • Dyspnea, fatigue, edema, orthopnea. • Palpitations, occasionally syncope. • Systemic and pulmonary emboli (+4 %/year.) • Atypical chest pain ( 1/3 of patients) • Physical Finding • Reflects the variable severity of CHF. • Diagnostic Studies • CXR, EKG, Echocardiogram (segmental vs global asynergy) • MRI (Dysplastic RV Cardiomyopathy) • Gallium 67 (sarcoidosis, myocarditis) • Cardiac Catheterization (r/o CAD, check pressures, usually biopsy not indicated.)
Posteroanterior CXR of a 52 y.o man with idiopathic dilated cardiomyopathy exhibit diffuse cardiomegaly. The LA can be seen as a faint double density.
Echocardiogram: Severe Dilated Cardiomyopathy Apical four-chamber echocardiographic view of a patient with severe dilated cardiomyopathy. All four cardiac chambers are markedly enlarged. The left ventricular ejection fraction was 22%, and the left ventricular end-diastolic diameter was 74 mm.
Dilated (Congestive) Cardiomyopathy • Endomyocardial Biopsy • Low diagnostic yield • Uncertainty regarding role of immunosuppressive therapy • Led most investigators to abandon it routine use
Endomyocardial Biopsy: Myocarditis A 19y.o. man; presented with DCM and VPCs. The findings of focal lymphocytic infiltrates, interstitial edema, and myocyte degeneration are typical of myocarditis. The patient responded to prednisone.
Biopsy: End-Stage Dilated Cardiomyopathy An 80 y.o. man with end-stage CM. There is marked hypertrophy of myocytes, interstitial and focal fibrosis,and no evidence of interstitial inflammation. Immunosuppressive therapy was not indicated.
Dilated Cardiomyopathy (DCM)Course and Prognosis • The most common complication of DCM is progressive CHF – the cause of death in 50 – 75% • Sudden death (SD) by arrhythmia is common especially in patients with complex ventricular ectopy and severe LV dysfunction. • Systemic / pulmonary embolism is found at autopsy in 50% of patients with DCM – emboli can cause catastrophic complications but rarely death. • Prognosis varies considerably from fulminent cases that result in death within a few weeks, or conversely some patients do remarkably well for years. Previously, most died within 5 years. • Spontaneous improvement in LV function occurs in 20 – 40%, most frequently within 6 months. • A peak 02 uptake less than 14 ml/kg /min predicts 1 year survival of 70%. Consider cardiac transplant if V02.
Survival in Symptomatic Idiopathic Dilated Cardiomyopathy Survival symptomatic IDC in seven reported series. Study A, 1986-89 (basis for selection unspecified); study B, 1975-84 (population based); study C, 1973-87 (referral based); study D, 1962-82 (referral based); study E, 1960-73 (referral based); study F, 1972-82 (referral based); study G, 1965-86 (autopsy series). (N number of patients)
Dilated Cardiomyopathy Medical Treatment • Limit activity based on functional status • Salt restriction of a 2gm Na+ (5gm NaCl) diet • Fluid restriction for significant low Na+ • Initiate combination medical therapy • ACE inhibitors (lisinopril, enalopril, captopril, etc.) Beta blockers (carvedilol, long acting metoprolol, bisoprolol) • Loop diuretics (toresemide, furosemide) for symptoms of fluid overload. • ARB (candesartan, valsartan) • Aldosterone blockers (spironolactone, eplerenone) • Digoxin (to treat symptoms) • Hydralazine / nitrate combination (if unable to tolerate ACE inhibition)
Dilated Cardiomyopathy Medical Treatment • Anticoagulation therapy is controversial in idiopathic cardiomyopathy. Consider with marked right sided failure and/or EF < 30. Use if embolic event has already occurred. • Antiarrhythmics: arrhythmias are common however, empiric antiarrhythmic drug therapy has been disappointing. Only amiodarone seems relatively safe but without clear mortality benefit in DCM.
Dilated Cardiomyopathy Device Treatment SAECG and EP are not reliable in assessing prognosis or guiding antiarrhythimic therapy in patients with DCM. • Defibrillator (AICD) is indicated in patients with cardiomyopathy and EF<30%. SCUD-Heft demonstrated mortality benefit in patients with EF<30% of either ischemic or nonischemic etiology. • Biventricular pacing restores synchronous LV contraction and decreases heart failure symptoms when used in combination with medical therapy. Used in combination with AICD. • If symptoms are still not controlled, may consider transplant.
Obstructive (HOCM. Labile and associated with mitral valve pathology.) Non Obstructive Concentric Mid ventricular Apical Hypertrophic Cardiomyopathy* * The vast majority of cases of hypertrophic cardiomyopathy result from specific defects in the genes regulating the formation of cardiac muscle This defect is either sporadic or hereditary in 50% of cases (autosomal dominant).
35% 10%
Hypertrophic Cardiomyopathy • The hallmark of the disease is unexplained myocardial hypertrophy or hypertrophy out of proportion to the hemodynamic load. • Frequently inherited with autosomal dominant transmission and highly variable penetrance. • In the obstructive form: ASH, SAM, MR. • Obstruction may be fixed or labile. • Hyper-contractile LV (EF 80 – 90%) with reduced ESV. • Reduced LV diastolic compliance. (cause of NEF-CHF) • Factors that provoke or increase/decrease obstruction: • Change in contractile state. • Change in chamber size (preload and after load)
Hypertrophic Cardiomyopathy • Usually assymetrical hypertrophy with the septum:posterior wall thickness >1.3:1.0 (although this may occasionally be seen in concentric hypertrophy.) • Apical and mid ventricular variants are unusual. The apical pattern may be characterized by giant T wave inversions on ECG. • Hypertensive HCM may be seen in elderly hypertensive pts and is characterized by severe concentric LVH out of proportion to the degree of hypertension.
Coronal Section in Hypertrophic Cardiomyopathy The thickening of the IVS is disproportionately greater than that of the LV wall behind the posterior mitral leaflet. The LV chamber is small and elongated.
Myofibrillar Pattern in HCM vs. HTN Different myofibril patterns in tissue taken from the septum of a patient with HCM (left) and from the hypertrophied LV of a patient with HTN (right). Note the chaotic arrangement of the cells of septal myocardium taken from the HCM.In contrast, note the orderly parallel arrangement of myofibrils in ventricular myocardium in the HTN patient.
Morphologic and Hemodynamic Characteristics of the Cardiomyopathies Dilated Hypertrophic Restrictive Obliterative(Restrictive-Obliterative) Morphologic Biventricular dilatation Marked hypertrophy of leftventricle and occasionallyof right ventricle; usuallybut not always,disproportionatehypertrophy of septum Reduced ventricularcompliance; usuallycaused by infiltrationof myocardium (e.g., byamyloid, hemosiderin,or glycogen deposits) Thickened endocardiumor mural thrombi, or both,act as space-occupyinglesions Homodynamic Cardiac output Normal Normal to Normal or Stroke volume Normal or ↑ Normal or Normal or Ventricular fillingpressure ↑↑ Normal or ↑ ↑↑ Usually ↑ Chamber size ↑↑ Normal or Normal or ↑ Typically Ejection fraction ↑↑ Normal to Normal to Diastolic compliance Normal or Other findings May have associatedfunctional mitral ortricuspid regurgitation Obstruction may developbetween interventricularseptum and septal leafletof mitral valveMitral regurgitation maybe present Characteristic ventricularpressure tracings thatresemble those recordedin constrictive pericarditis,with early diastolic dip-and-plateau configuration May be seen as a featureof the hypereosinophilicsyndromesSome investigators considerit a form of restrictivecardiomyopathy
Hypertrophic Cardiomyopathy Pathophysiology • Systole • Dynamic outflow tract gradient. May not be present at rest but may provoke with standing, exercise or inotropic drugs. • Diastole • Impaired diastolic filling, filling pressure of LV. • Myocardial ischemia • Muscle mass, filling pressure, O2 demand • Coronary vasodilator reserve, capillary density • Abnormal intramural coronary arteries with systolic compression of arteries.
Survival Curves in Hypertrophic Cardiomyopathy The survival of patients with hypertrophic cardiomyopathy caused by different mutations: cardiac troponin T mutations (introns 15 G1(r) A, Ile79Asn, DGlu160, and Arg92Gln) is similar to that in persons with a malignant b-myosin heavy-chain mutation (Arg403Gln) but significantly shorter than that observed in persons with a benign myosin mutation (Val606Met).
Factors That Increase Obstruction Factors That Decrease Obstruction Mechanism Physiologic or Pharmacologic Factor Mechanism Physiologic or Pharmacologic Factor Increase incontractility Digitalis glycosidesBeta-adrenergic stimulation (e.g., isoproterenol,epinephrine)TachycardiaPremature beats Decrease incontractility Beta-adrenergic blockade (e.g., propranolol)Heavy sedation and general anesthesiaCalcium channel blockers, disopyramide, and otherdrugs that depress myocardial function Reduction inpreload Valsalva maneuver†Decrease in intravascular volume (e.g., from hemorrhage,diuresis, GI losses)Standing†Nitroglycerin and related drugs†Vasodilator drugsTachycardia Increase inpreload Intravascular volume expansionSquatting†BradycardiaBeta-adrenergic blockade Reduction inafterload HypovolemiaNitroglycerin and related drugs†Vasodilator drugs Increase inafterload Intravascular volume expansionSquatting†Alpha-adrenergic stimulation (e.g., phenylephrine,mephentermine)Handgrip exercise† Factors That Influence the Degree of Obstruction in Hypertrophic Cardiomyopathy* *In general, anything that increases obstruction will increase the intensity of the associated murmurs, whereas factors that reduce obstruction will diminish murmur intensity.†May assist in diagnosis at the bedside.
Hypertrophic Cardiomyopathy Diagnosis • Symptoms • Angina (Recumbent position) • Syncope (After exercise, arrhythmia) • Palpitations (AF, VT) • CHF (Loss of atrial contraction, AF with fast response) • Systemic embolism • Sudden Death. (Even in asymptomatic patients.) Lethal arrhythmia more likely in young. • Physical examination • EKG (May have LVH pattern, preexcitation, abnormal Q waves, giant T waves.) • Echocardiography (LVH concentric, apical, ASH, septum:posterior > 1.3:1, SAM, “lobster claw” outflow tracing.) • Cardiac Cath (Pressure tracings demonstrating outflow tract obstruction.)
Changes of Murmer in Obstructive Hypertrophic Cardiomyopathy Variations in the quality of the murmur associated with HOCM are observed before (a), during (b), and after (c) the Valsalva maneuver. Before the Valsalva maneuver, a soft systolic murmur is recorded at the apex. The arterial pulse contour is normal. During the Valsalva maneuver, there is a dramatic increase in the intensity of the murmur. After Valsalva release, the murmur becomes softer, but the carotid pulse exhibits the classic spike-and-dome configuration characteristic of obstructive hypertrophic cardiomyopathy.
Hypertrophic Cardiomyopathy Increase in Gradient and Murmur Contractility Preload Afterload Valsalva (strain) -- ↓standing -- --postextrasystole -- isoproterenol digitalis --amyl nitrite - ↑ ↑ nitroglycerin -- exercise tachycardia --hypovolemia
Hypertrophic Cardiomyopathy Decrease in Gradient and Murmur Contractility Preload AfterloadValsalva (overshoot) -- ↑ ↑ squatting -- ↑passive leg elevation -- --phenylephrine -- -- beta-blocker ↑ -- general anesthesia -- --isometric grip -- --
HypertrophicCardiomyopathyHCM vs Aortic Stenosis HCM Fixed Obstruction carotid spike and dome parvus et tardus murmur Valsalva, standing radiates to carotids squatting, handgrip passive leg elevation systolic thrill4th left interspace 2nd right interspace systolic clickabsent present
ECG in Obstructive Hypertrophic Cardiomyopathy Abnormal Q waves suggestive of an old anterior myocardial infarct are observed in leads V3 through V6 in an ECG recorded in a 45-year-old woman with obstructive hypertrophic cardiomyopathy.