Download
1 / 67
680 likes | 941 Views
The Patient with Low HDL Cholesterol. James A. Underberg, MD, MS, FACPM, FACP, FASH,FNLA Preventive Cardiovascular Medicine Clinical Assistant Professor of Medicine Division of General Internal Medicine, NYU Medical School & NYU Center for Prevention of Cardiovascular Disease

E N D
The Patient with Low HDL Cholesterol James A. Underberg, MD, MS, FACPM, FACP, FASH,FNLA Preventive Cardiovascular Medicine Clinical Assistant Professor of Medicine Division of General Internal Medicine, NYU Medical School & NYU Center for Prevention of Cardiovascular Disease Director Bellevue Hospital Primary Care Lipid Clinic ASH Hypertension Specialist Diplomate American Board of Clinical Lipidology Fellow Society of Vascular Medicine & Biology Specialist
Disclosures • Honoraria for Speakers Bureau (Pharma) : AstraZeneca, Abbott, Forest, GlaxoSmithKline, Daiichi-Sankyo, Kowa, Novartis, Pfizer, Liposcience, diaDexus, Merck, Eli Lilly • Honoraria for CME Programs :American Heart Association, National Lipid Association, American College of Reproductive Medicine, PriMed, Primary Care Network • Consulting Income: Liposcience, News Corporation, Publicis Inc., Summer Street Consulting Inc. Guidepoint Global • Advisory Boards: Kowa, Abbott, Merck • Clincial Research Funding: Genzyme, GlaxoSmithKline, • Medical Education Committee Member : NAMS, ASH, NLA • Editoral Board Member: Journal of Clinical Lipidology
Case#1 • 52 year old male presents with one week of shaking chills, fever, and sweats • He has lost 12 lbs over the past 6 weeks without change in diet or exercise • He denies cough, urinary symptoms or change in bowel habits • He does note a decrease in his appetite • Who would like to give him aspirin for the fever and send him home?
Case #2 • 41 year old white male presents for evaluation of low HDL cholesterol ( HDL-C) • No significant past medical history • Physical exam unremarkable. Normal BP, BMI 23.4 WC 32” • Father with MI age 51, died age 52 sudden death. Was a smoker, never told he had a lipid disorder. • Patient does not drink alcohol, and does not smoke, He exercises 4 times a week and eats mostly fish and vegetables, salad. Small amounts of lean meat and poultry.
Case #2 • Lab Evaluation • Total Cholesterol 140 mg/dl • HDL-C 21 mg/dl • LDL-C 94 • TG 125 mg/dl • FBS 90 mg/dl, HbA1c 5.2% • Bun/Cr. 15/0.9 LFT and all other labs WNL
Measures of HDL ( High density Lipoprotein) • HDL-C : Concentration of cholesterol Contained in HDL Particles • HDL-P : Concentration of HDL Particles that carry cholesterol • Apo A1: Concentration of Apo A1 (building block of HDL) number of molecules of Apo A1 can vary per HDL particle • Why is this important? • Measures of HDL Functionality
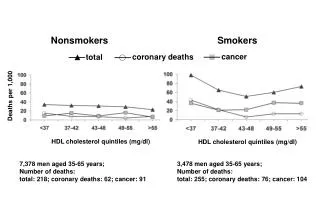
CHD Incidence Related to HDL-C Levels in Various Trials CHD incidence Women Men 0 -2 -4 % change in risk per 1 mg/dL increment in HDL-C -6 -8 -10 FHS LRCF CPPT MRFIT LRCF FHS 95% confidence intervals (CIs) for adjusted proportional hazards regression coefficients. FHS = Framingham Heart Study; LRCF = Lipid Research Clinics Prevalence Mortality Follow-up Study; CPPT = Lipid Research Clinics Coronary Primary Prevention Trial; MRFIT = Multiple Risk Factor Intervention Trial Gordon DJ et al. Circulation 1989;79:8–15
CAD Risk as a Function of LDL-C and HDL-C in Men (Ages 50 to 70 Years Old): Framingham Heart Study mmol/L mg/dL Coronary Artery Disease (CAD) Relative Risk 25 0.65 45 1.16 65 1.68 HDL Cholesterol (HDL-C) 85 2.2 220 160 100 mg/dL 5.69 4.14 2.58 mmol/L LDL Cholesterol (LDL-C) Reprinted from Castelli WP. Can J Cardiol. 1988;4: 5A–10A, with permission from Pulsus Group Inc.
HDL-C Emerging Risk Factors Collaboration Coronary Heart Disease 3.5 HDL-C 3.0 2.5 2.0 Hazard Ratio 1.5 1.0 0.8 30 40 50 60 70 80 Usual Mean Level, mg/dL Emerging Risk Factors Collaboration. JAMA. 2009;302(18):1993-2000.
Hazard Ratios for Coronary Heart Disease Across Fifths of Usual Lipids or Apolipoproteins 3.0 Non-HDL-C Apo B HDL-C Apo AI 2.5 2.0 1.5 Hazard Ratio 1.0 0.8 0.5 -1.0 -0.8 -0.6 -0.4 -0.2 0 0.2 0.4 0.6 0.8 1.0 1.2 Quintile Mean (SD Distance from Overall Mean) Emerging Risk Factors Collaboration. JAMA. 2009;302(18):1993-2000.
Meta-Analysis: Predictive Value of HDL-C • Coronary Primary Prevention Trial (CPPT) • Multiple Risk Factor Intervention Trial (MRFIT) • Lipid Research Clinics Prevalence Mortality Follow-up Study (LRCS) • Framingham Heart Study (FHS) 1 mg/dL Increase in HDL-C CPPT MRFIT LRCS LRCS FHS FHS 3% CHD Risk in Women 2% CHDRisk in Men Gordon DJ, et al. Circulation. 1989;79:8-15.
Evaluation of Low HDL-C • Low HDL-C has many etiologies • While population data suggests that low HDL is associated with increased risk of CHD events , many examples exist of patients with low HDL-C levels - no CHD and patients with increased HDL-C levels that present with CHD
HDL-C Levels Often Do NotPredict ASHD • Torcetrapib • ApoA-1 Milano • WHI Estrogen • SRB1 rodent data • LCAT deficiency • Tangier Disease
High HDL-C decreases cardiovascular risk at low LDL-C (<70 mg/dL) – TNT study 39% lower risk Risk of major cardiovascular events over 5 years (%) _ HDL cholesterol (mg/dL) Barter PJ, Gotto AM, LaRosa JC et al. HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events. N Engl J Med 2007; 35727.
Risk Factors for Coronary Artery Disease in Patients With Elevated High-Density Lipoprotein Cholesterol Database Review (n=1610) Chart Review (n=196) * * * * Normal HDL-C Orange High HDL-C Blue Defaria Yeh D, et al. Am J Cardiol. 2007;99(1):1-4.
A-I Antioxidant + Nitric Oxide Antithrombotic Endothelial Integrity Antiinflammatory Pro-fibrinolytic Macrophage Reverse Cholesterol Transport HDL Functionality and Vascular Protection None of these effects have a direct relationship to HDL-C or HDL particle size
Dysfunctional HDL-C Factors that can make the “good” cholesterol better – or worse • Proven to promote the anti-inflammatory effect of high-density lipoprotein (HDL) • Apolipoprotein (apo) A-I mimeticsa • Exercise, low-fat diet • Polyunsaturated fat diet • Statins • May promote HDL’s anti-inflammatory effect • Antirheumatic biologicals • Apo A-IMilanoa • Delipidated HDLa • Promote proinflammatory HDL • Coronary atherosclerosis • Diabetes mellitus • Hemodialysis • Diet high in saturated fat • Infection • Rheumatoid arthritis • Surgery • Systemic lupus erythematosus a Currently in development Ansell BJ. Cleve Clin J Med. 2007;74(10):697-700, 703-705.
Acute Phase HDL effects during inflammaton or autoimmune disorders Atherosclerosis 220 (2012) 11–21
Cholesterol Efflux Capacity N Engl J Med 2011;364:127-35.
HDL-C Levels vs. Functionality • At no time can a man say “It is,” only “ I believe it was," and “I hope it shall be." Transformation is the only constant. From earth we come and to earth we shall return, but while above it we shall be shapeless, unsettled, as water. -Tandou Armah Cisse, So Far, So Far from Home
Lipid levels in patients hospitalized with coronaryartery disease: An analysis of 136,905 hospitalizationsin Get With The Guidelines AmitSachdeva, MD,a Christopher P. Cannon, MD,bPrakash C. Deedwania, MD,c Kenneth A. LaBresh, MD,d Sidney C. Smith, Jr, MD,e David Dai, MS,f Adrian Hernandez, MD,f and Gregg C. Fonarow, MD a on behalf of the GWTG Steering Committee and Hospitals Los Angeles and San Francisco, CA; Boston and Waltham, MA; and Chapel Hill and Durham, NC (Am Heart J 2009;157:111-7.e2.)
Total Cholesterol 174 LDL 104 HDL 39 TG 161 Average BMI 28.9 HTN 54.2 (Am Heart J 2009;157:111-7.e2.)
LDL Particles LDL Particles (nmol/L) LDL Cholesterol HDL Cholesterol (mg/dL) Low HDL-C is associated with increased LDL-Particle #, Apo B and Non-HDL-c Cromwell WC and Otvos JD. CurrAthero Reports 2004;6:381-387
Association of HDL-C With CHD Events, by Apolipoprotein B100 Tertile CHD event rate per 1000 PYs HDL-C Quintile Apolipoprotein B100 Tertile Modified from :Ann Intern Med. 2011;155:742-750.
Differential Dx of Low HDLc • Diagnosis often imparts risk or lack thereof • Diagnosis help to understand need for treatment • Diagnosis helps to understand how aggressive treatment should be • Diagnosis helps guide the management other secondary causes of low HDL-C
Causes of Low HDL-C • Lifestyle • Diet • Smoking • Medications • Secondary Disease States • Genetic disorders
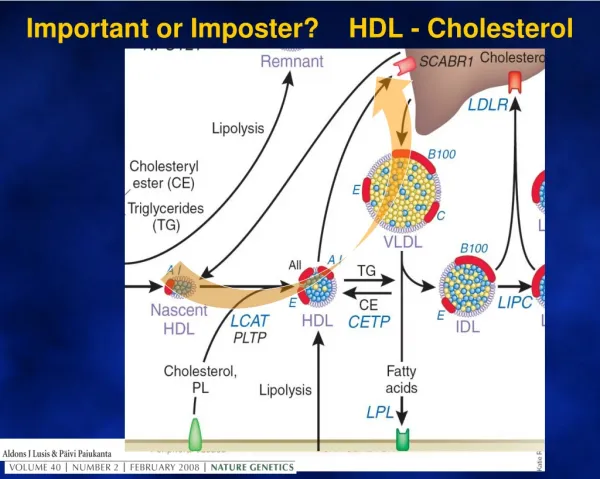
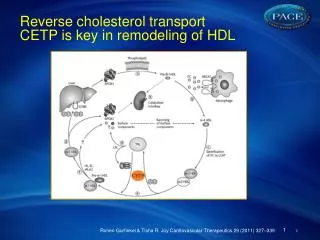
Cholesterol ester Triglyceride Small HDL Hepatic Lipase The most common cause of depressed HDL is secondary to insulin resistance, increased flux of FFA to the liver, VLDL overproduction, and the subsequent formation of low levels of HDL in conjunction with elevated TG and increased small, dense LDL particles. TG CETP CE Otvos JD, et al. Am J Cardiol.2002;90(8A):22i-29i
Acquired Diseases CausingHDL-C Deficiency Biliary cirrhosis, liver failure, liver congestion Liver diseases Inflammatory enteropathies General inflammations (smoking) Hematological disease Drugs & hormones Crohn’s Disease Systemic inflammation response syndrome, sepsis, burns Histiocytosis, Hodgkin’s lymphoma, plasmacytoma Androgens, certain progestins, anabolics, probucol Adapted from von Eckardstein A. Atherosclerosis.2006;186:231-239
HDL-C Deficiency Table 1: Common Causes of High-density Lipoprotein Deficiency • Obesity, especially visceral obesity • Insulin resistance • Hypertriglyceridemia • Metabolic syndrome • Type 2 diabetes • HIV disease • Low fat intake or diets enriched with polyunsaturated fat • Cigarette smoking • Severe stress states, e.g., sepsis, burns • Liver disease • Renal insufficiency • Drugs • Isotretinoin • Sirolimus (rapamycin) • Protease inhibitors • Androgenic steroids • Non-selective β-blockers • Probucol • Recombinant interleukin-2 Brown BG, et al. J Clin Lipidol. 2007;1(1):88-94.
HDL-C Deficiency Table 2: Causes of Severe High-density Lipoprotein Cholesterol Deficiency • Moderate to severe hypertriglyceridemia • Critical illness, including sepsis, burns, small bowel exclusion • Anabolic steroids • Acquired LCAT deficiency, possibly decreased ApoA-Isynthesis • Severe cholestasis • Cholestatic liver disease with liver failure • Alcoholic hepatitis • Acute viral hepatitis • Alcoholic cirrhosis • Partial hepatectomy (temporary) • Recombinant interleukin-2 therapy • Disappearing HDL syndrome • PPAR agonists – idiosyncratic reaction • PPARγ(thiazolidinediones) • PPARα(fibrates) • Paraproteinemia • True deficiency • Artifactual deficiency * Apo-AI, apolipoprotein A-I; HDL, high-density lipoprotein; LCAT, lecithin cholesteryl acyl transferase; PPAR, peroxisome proliferation-activated receptor. Brown BG, et al. J Clin Lipidol. 2007;1(1):88-94.
Severe High-density Lipoprotein Cholesterol (HDL-C) Deficiency Occurring with the Introduction of Fenofibrate Therapy in a Patient With Diabetes and Hypertriglyceridemia Rosiglitazone Metformin Gemfibrozil Fenòfib Fenòfib 300 50 40 Triglyceride mg/dL 200 30 HDL-C mg/dL 20 100 10 7/06 8/06 9/06 10/06 11/06 2002 2003 2004 2005 2006 2007 Brown BG, et al. J Clin Lipidol. 2007;1(1):88-94.
Formation & Conversion of HDL Hyper-triglyceridemia Lipid-storage diseases Obesity Hormones Diabetes mellitus Genetic Factors with Low HDL-C HDL-deficiency von Eckardstein, A. Atherosclerosis 2006;186:231-239
Genetic HDL Disorders No clinical value: monogenic dis. rare, polygenic not understood Alawadhi M,et al. Curr Atheroscler Rep. 2005;7:196-203.
Hypoalphalipoproteinemias: Deletions and Non-sense Mutations in ApoA-I: Result in little if any biosynthesis of apoA-I by liver and intestines – early CVD – may also see peripheral cholesterol deposition – cataracts, planar xanthomas. Missense Mutations in ApoA-I: Result in low HDL, but impact on CVD less clear. Example: Apo-AI Milano results from a mutation in the apoA-I gene at codon 173, Arg to Cys, and alters the structure of apoA-I heterozygotes have low HDL due to increased turnover of apoA-I, but surprisingly manifest little CVD. Disorders of HDL Metabolism
Hypoalphalipoproteinemias: Tangier Disease: Results from a defect in cholesterol and PL efflux from cells to apoA-I. Poorly lipidatedapoA-I is then rapidly removed by the kidney. Basic defect is in double dose mutation in ABCA1 gene. HDL markedly abnormal. Chylomicron-like particles are sequestered by the reticular endothelial cells (yellow tonsils). Early atherosclerosis is not a major feature. Disorders of HDL Metabolism
Hypoalphalipoproteinemias: LCAT Deficiency and Fish Eye Disease: Free cholesterol must be esterified to produce a spherical HDL; esterification is achieved via LCAT. Patients with LCAT deficiency have markedly reduced HDL. (Other lipoproteins are also abnormal). Clinical findings include glomerulosclerosis, normochromic anemia, and corneal opacities. Although CAD is not prominent, it has been reported. Classic LCAT deficiency – both α and β LCAT deficient – all lipoproteins abnl. If only α LCAT is abnormal – fish eye disease – a major finding is corneal opacities. Disorders of HDL Metabolism
Severe HDL-C Deficiency Syndromes Table 1: Characteristics of homozygotes in kindreds with severe high-density lipoprotein deficiency Apo, apolipoprotein; HDL-C, high-density lipoprotein cholesterol; LCAT, lecithin cholesteryl acyl transferase;LDL-C, low-density lipoprotein cholesterol. * Increased risk of developing renal failure, see references 31, 37, and 48. Santos RD, et al. J Clin Lipidol. 2008;2(4):237-247
Homozygous Familial Apolipoprotein deficiency tubo-eruptive xanthomas planar xanthomas tubo-eruptive xanthoma microscopy moderate corneal opacification Normal eye fundus Current Opinion in Lipidology 2010, 21:289–297
Enlarged orange tonsils from apatient with homozygous Tangier disease Current Opinion in Lipidology 2010, 21:289–297
LCAT remains a potential target JACC Vol. 58, No. 24, 2011 December 6, 2011:2488–90
A low HDL-C level is strongly and inversely associated with CHD risk The independent relationship holds after correction for other risk variables in multivariate analysis A low HDL-C level often correlates with elevations of serum triglycerides and remnant lipoproteins HDL may be antiatherogenic Promotes reverse cholesterol transport (RCT) Antioxidant and antiinflammatory properties inhibit atherogenesis NCEP ATP III: HDL-C Is an Independent Risk Factor for CHD Third Report of the NCEP Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III). Circulation. 2002;106:3143-3421.
National CholesterolEducation Program Adult Treatment Panel III NCEP-ATP III 2004 Addendum Grundy SM, et al. Circulation.2004;110:227-239
ADA/ACC 2008 Consensus Statement:Treatment Goals in Patients With Cardiometabolic Risk and Lipoprotein Abnormalities “In individuals on statin therapy who continue to have low HDL-C or elevated non–HDL-C, especially if Apo B levels remain elevated,combination therapy is recommended.” aMajor risk factors beyond dyslipidemia include smoking, hypertension, and family history of premature CHD. Brunzell JD, et al. Diabetes Care. 2008;31:811-822.
EAS Dyslipidemia Guidelines Lipid screening for CVD risk Characterization of dyslipidaemias before treatment European Heart Journal (2011) 32, 1769–1818
Recommendations for lipid analyses astreatment target in the prevention of CVD European Heart Journal (2011) 32, 1769–1818
Effects of Diet on HDL-C Siri-Tarino PW. Curr Atheroscler Rep. 2011;13(6):453-460.
Lifestyle Modification on HDL-C Singh IM, et al. JAMA. 2007;298(7):786-798
Currently Availablel HDL Raising Lipid Medications • Statins 5-10 % • Fibrates 10-20% • Niacin 20-30% • Bile Acid Sequestrants 3-5% • Thiazolidinediones (TZD) 5-10% JAMA, August 15, 2007—Vol 298, No. 7
Cholesteryl ester transfer protein (CETP) inhibitors Recombinant apolipoprotein A-I Reconstituted HDL Synthetic HDL particles LXR Agonists Developmental treatments for raising HDL cholesterol